- 1.0 Cross-Disciplinary Perspectives at 2026 bio: Why Viewing AAIC Through the AACR’s “Oncology Lens” Matters
- 2.0 London Review: Core Technical Topics of the 2026 bio Annual Meeting and the Evolutionary Path of Next-Generation Macromolecules
- 3.0 Cross-disciplinary Exploration at 2026 bio: Potential Intersections of ADCs, Nucleic Acid Therapeutics, and Combination Therapies in Neurodegenerative Diseases
- 4.0 Attending 2026 bio: How Participants Can Maximize the “Upstream and Downstream Support” Traffic Peak at AAIC
- 5.0 Summary and Outlook: Investment and R&D Trends in the Global CNS Sector After 2026 bio
- 6.0 2026 bio: Frequently Asked Questions (FAQ)
- 7.0 Disclaimer
Cross-Disciplinary Perspectives: An In-Depth Analysis of the AAIC 2026 Annual Meeting in London — A 2026 bio Deep Dive
From AACR Oncology to the Multimodal Therapy Revolution in Neurodegenerative Disease neurodegenerative disease research 2026 s
Author: https://bio-conference.com/ Editorial Team | Publication Date: July 2026 | Categories: AAIC 2026 · Neurodegenerative Disease neurodegenerative disease research 2026 s · Macromolecular Drugs
1.0 Cross-Disciplinary Perspectives at 2026 bio: Why Viewing AAIC Through the AACR’s “Oncology Lens” Matters

In July 2026, the Alzheimer’s Association International Conference (AAIC 2026)—the most prestigious annual gathering in the global neuroscience field—will officially open at the ExCeL London exhibition center.Thousands of researchers, clinicians, pharmaceutical BD teams, and investors will converge on the banks of the Thames, eager to capture firsthand signals of the next wave of breakthroughs in neurodegenerative disease R&D.
However, to truly understand what will unfold at this year’s London conference, expertise in neuroscience alone is far from sufficient. In the first half of 2026, the global narrative in biopharmaceuticals has quietly undergone a profound paradigm shift. This shift began precisely in oncology—specifically, at the American Association for Cancer Research (AACR) Annual Meeting held in San Diego this past April.
This article will begin by examining the trends emerging from AACR 2026, systematically tracing the origins and development of this paradigm shift, and illustrating how it illuminates—with remarkable precision—the current homogenization crisis facing neuroscience drug R&D. Only by understanding this can you truly grasp why the technical agenda of the AAIC 2026 London conference has taken its current form, and why these specific research directions are precisely the ones most worthy of attention.
1.1 The Dramatic Shift in the Biopharmaceutical Narrative in Q2 2026: The Transition from Single-Target Monoclonal Antibodies to Multi-modal Approaches
If we were to summarize the strategic focus of global multinational pharmaceutical companies in the first half of 2026 in a single sentence, it would likely be this: a shift from “single-target dominance” to “multi-dimensional assault.”
This is not mere rhetoric, but an industry assessment backed by actual M&A data and clinical trial designs. Take the oncology sector as an example: GSK, Bristol-Myers Squibb (BMS), and BioNTech intensively completed a series of acquisitions targeting “multi-modal”pipelines—the term “multimodal” refers to innovative therapies that integrate two or more mechanisms of action, including bispecific antibod central to any CNS bispecific antibody pipeline ies, antibody-drug conjugates (ADCs), and combination regimens with immune checkpoint inhibitors.
[Industry Background Tip] In April 2026, among the more than 2,000 research presentations at the AACR 2026 Annual Meeting in San Diego, the frequency of the search term “Bispecific ADC” increased by more than 14-fold compared to AACR 2021 five years prior;while the search term “Combination therapies” increased nearly sevenfold. This is not merely a conceptual trend, but a lagging signal indicating that the academic community is finally catching up after capital and R&D resources have already been reallocated.
1.1.1 Lessons from the Recent AACR 2026: The Logic Behind Global Pharmaceutical Giants’ “Frenetic Acquisition Spree”
Before explaining why multinational pharmaceutical giants are “on a frenzied buying spree” for multimodal pipelines, we must first clarify a fundamental logic: what risks are they seeking to mitigate?
Over the past decade, the core narrative of cancer immunotherapy has been PD-1/PD-L1 monoclonal antibodies—Keytruda and Opdivo. The combined peak annual global sales of these two drugs exceed $30 billion, having single-handedly reshaped the global landscape of cancer drugs. However, as we enter 2024–2025, the cracks in this rosy story are becoming increasingly difficult to ignore.
The data doesn’t lie. In clinical practice, over 60% of solid tumor patients have an initial response rate of less than 30% to PD-1 monoclonal antibody monotherapy; more critically, even among initial responders, the secondary resistance rate within 12–18 months reaches as high as 40–60%.In other words, the historical mission of PD-1 inhibitors has largely been fulfilled—they opened the door to immunotherapy, but they cannot complete the journey alone.
Against this backdrop, GSK’s collaborations with several innovative Chinese pharmaceutical companies are particularly significant.Take the novel B7-H3/PTK7 dual-target ADC pipeline as an example: the B7-H3 target is highly expressed on the surface of various solid tumor cells, while PTK7 is directly associated with the migration and invasion capabilities of tumor cells. The design logic behind this pipeline is based on the premise that “eliminating a single target is far from sufficient,” aiming to simultaneously block two critical cancer cell survival pathways.
Table 1-1: Summary of M&A and Collaborations for Multimodal Pipelines by Major Multinational Pharmaceutical Companies from Q4 2025 to Q1 2026
| Multinational Pharmaceutical Company | Type of M&A/Collaboration Target | Core Technology Tags | Strategic Intent |
| GSK | B7-H3/PTK7 Dual-Target ADC (in collaboration with a Chinese pharmaceutical company) | Bispecific ADC, multi-target coverage | Avoids resistance to single-target PD-1 inhibitors and builds a differentiated oncology pipeline |
| BMS | Multiple Phase I/II clinical programs combining bispecific antibodies with PD-1 | Bispecific Antibody + Immunotherapy Combination | Adding precision targeting to existing checkpoint inhibitors |
| BioNTech | mRNA-encoded bispecific antibody technology platform (acquired from a European biotech company) | mRNA macromolecular platform | Extending mRNA delivery logic from vaccines to antibody therapeutics |
| Eli Lilly | GPRC5D/BCMA bispecific antibody (for multiple myeloma) | Bispecific T-cell conjugate | Addressing the gap in CAR-T therapy coverage for solid tumors |
| AstraZeneca | Third-generation ADC linker technology platform (multiple INDs) | Novel cleavable linkers and bystander effect optimization | Extending the precise release window of ADC payloads in the tumor microenvironment |
As clearly shown in the table above, the key factor in this round of M&A is not “strength,” but “integration”—the ability to organically integrate two or more killing mechanisms into a coherent therapeutic strategy is the bottom-line criterion determining whether multinational giants are willing to invest.This logic of “combination” does not simply involve using two drugs together; rather, it involves “physically binding” two mechanisms of action together at the molecular design level—one molecule, two warheads, a single administration, and simultaneous inactivation of two targets. This is the revolutionary aspect of bispecific ADCs.
Looking ahead to AAIC 2026, the greatest significance of this logic lies in the fact that the next generation of macromolecular drugs in neuroscience is accelerating its catch-up along the same path in oncology—from monoclonal antibodies to bispecific antibod central to any CNS bispecific antibody pipeline ies and ADCs. The 2026 AAIC conference in London will likely serve as the historic stage where we witness this catch-up “crossing the inflection point.”
1.1.2 The Surge in Combination Therapies of Bispecific Antibody-Drug Conjugates (ADCs) and Immune Microenvironment Modulation: The Industry-Wide Solution to Resistance and Target Limitations of First-Generation Drugs
First-generation ADC drugs, represented by DS-8201 (trastuzumab deruxtecan, T-DXd, trade name Enhertu), generated nearly mythical clinical data between 2020 and 2024.In the field of HER2-positive breast cancer, the objective response rate (ORR) of DS-8201 as a monotherapy exceeded 70%, and its efficacy extended to HER2-low and even HER2-ultralow subgroups.
However, a systematic review published in the October 2025 issue of *Nature Medicine* revealed a warning sign that has put the industry on high alert:Among HER2-positive breast cancer patients treated with DS-8201 for more than 18 months, the incidence of drug resistance continued to accumulate at a rate of 4–6% per month, and the mechanisms of resistance exhibited high heterogeneity, making it difficult to explain them with a single mechanism. This implies that while the clinical value of DS-8201 is undeniable, it is not the end of the story.The “Achilles’ heel” of first-generation ADCs will begin to emerge in 2025–2026.
[Industry Background Tip] A review published in the March 2026 issue of *Lancet Oncology* notes that, in response to the drug resistance issues gradually emerging in global multicenter clinical trials of DS-8201, the research community is currently debating two primary strategies: First, using bispecific antibod central to any CNS bispecific antibody pipeline ies to simultaneously block HER2 and another resistance-associated escape target (such as HER3 or MET);Second, using immune microenvironment modulators (such as PD-1/VEGF bispecific antibodies) to reshape the “immune desert” surrounding the tumor, enabling the payload released by the ADC to achieve greater killing efficiency with the assistance of activated immune effector cells.
Both approaches point toward the same goal: combination sensitization—broadening the ADC’s therapeutic coverage through combination therapy or intramolecular dual-target design, while simultaneously mobilizing the synergistic power of the immune system to address the core issue of “drug-resistant tumor cells surviving after the payload has been delivered.”
Table 1-2: Summary of Mainstream Technical Approaches for ADC Combination Sensitization (Q2 2026 Perspective)
| Combination Strategies | Technology Combinations | Core Scientific Logic | Representative Clinical Programs (as of Q2 2026) |
| Dual-Target ADC | ADC-conjugated bispecific antibodies (Bispecific ADC) | Simultaneously blocks two targets, preventing cancer cells from escaping by upregulating alternative targets | GSK-B7H3/PTK7 ADC (Phase I/II), AZ-MET/HER2 Bispecific ADC (IND) |
| ADC + PD-1 Bispecific Antibody Combination | ADC + Immuno-Oncology bispecific antibody | The payload induces immunogenic cell death (ICD), while the bispecific antibody simultaneously activates the T-cell response | DS-8201 + Pembrolizumab (multiple registrational studies) |
| ADC + VEGF neutralization | ADC + Anti-angiogenic bispecific antibody | Inhibits tumor angiogenesis and increases ADC intratumoral penetration | T-DXd + Bevacizumab (Ovarian Cancer) |
| Immune microenvironment modulation + ADC | TREM2 Inhibitor/CCR2 Antagonist + ADC | Eliminates M2 tumor-associated macrophages, shifts the immunosuppressive microenvironment to a pro-inflammatory state, and enhances the cytotoxic efficacy of the ADC payload | Multiple Phase I exploratory studies (to be initiated in the first half of 2026) |
| Upstream silencing of nucleic acid therapeutics + ADC | siRNA/ASO silencing of drug-resistant genes + ADC | Preemptively block the expression of resistance genes (e.g., MRP1/BCL-2) at the transcriptional level via RNAi, thereby neutralizing the innate defense mechanisms of resistant cells against the ADC payload | Preclinical/Early Phase I (partially led by Chinese biotech companies) |
As shown in the table above, “combination sensitization” is no longer merely an academic hypothesis but a comprehensive R&D strategy spanning multiple targets and various technical approaches.This shift in understanding holds even more profound implications for the field of neuroscience than for oncology—because neurodegenerative diseases (such as Alzheimer’s disease) face not only insufficient coverage of single targets but also the more complex “physical delivery barrier of the blood-brain barrier (BBB).”
1.2 The “Historic Leap” and “Hitting the Wall” in CNS Macromolecular Drugs
In July 2023, the U.S. FDA officially approved lecanemab (brand name Leqembi), jointly developed by Eisai and Biogen, for the treatment of early-stage Alzheimer’s disease (AD).Following aducanumab (Aduhelm), this marks another anti-β-amyloid (Aβ) monoclonal antibody to receive traditional FDA approval. Leqembi’s approval was based on a Phase III randomized controlled trial (CLARITY-AD) involving nearly 1,800 participants and18-month Phase III randomized controlled trial (CLARITY-AD), demonstrating a statistically significant slowing of cognitive decline on the primary clinical endpoint (change in CDR-SB score).
In early 2024, Eli Lilly’s donanemab reported even more impressive data from its Phase III clinical trial (TRAILBLAZER-ALZ 2), achieving a clinical benefit of up to a 35% reduction in CDR-SB progression in the early-stage AD subgroup, and received FDA approval for marketing in the second half of 2024 (brand name Kisunla).However, following this breakthrough, the industry rapidly entered a period of sober reflection in 2025–2026.
1.2.1 Reflections During the “Cooling-Off Period” Following the Successful Market Launch of Eisai/Biogen’s Leqembi and Eli Lilly’s Donanemab: The Marginal Benefits of Monotherapy Targeting β-Amyloid (Aβ)
The market launches of Leqembi and Kisunla did not result in the explosive growth anticipated by the public. Ultimately, the reason points to a single core contradiction: in the view of most clinicians and health insurance agencies, the cost-effectiveness—the balance between the absolute clinical benefit and the treatment costs and safety risks—has not yet reached the threshold for widespread adoption.
Take the CDR-SB score as an example—one of the primary clinical endpoints currently used to measure cognitive decline in Alzheimer’s disease, where a higher score indicates worse cognitive function. In the CLARITY-AD trial, the CDR-SB change in the Leqembi group was 0.45 points lower than in the placebo group (18 months, full analysis set).While statistically significant, whether a 0.45-point difference is “visible and perceptible” to patients’ families and treating physicians remains a subject of ongoing debate within the neuroscience community.
Table 1-3: Comparison of Key Clinical Data for Leqembi and Kisunla with Current Treatment Limitations (Q1 2026 Perspective)
| Drug | Clinical Trial | Primary Endpoint (CDR-SB) Improvement | Annual Treatment Cost (U.S. Market) | Key Safety Concerns |
| Leqembi (lecanemab) | CLARITY-AD (N=1,795) | 27% reduction (0.45-point difference) | Approx. $26,500/year | ARIA-E (12.6%), ARIA-H (17.3%) |
| Kisunla (donanemab) | TRAILBLAZER-ALZ 2 (N=1,736) | 35% reduction in the early subgroup | Approx. $32,000/year | ARIA-E (24%), ARIA-H (31.4%) |
| Conventional standard therapy (cholinesterase inhibitors) | Long-term clinical practice | No substantial change in cognitive progression | Approx. $2,000–$5,000/year | Gastrointestinal side effects, effects on heart rate |
Concerns about diminishing returns have become a pervasive sense of uncertainty in the neuroscience community in 2025–2026. Is clearing Aβ plaques a necessary condition for halting Alzheimer’s disease, or is it a sufficient condition? If it is merely a necessary condition, then all existing drugs can achieve is “clearing a key piece of evidence, but the culprit remains.” It is precisely this sense of uncertainty that is driving the neuroscience community to rapidly pivot toward “multi-target combination” approaches—a shift that mirrors exactly the pivot the oncology community underwent after encountering resistance to first-generation ADCs.
1.2.2 Common Clinical Pain Points: The “Drug Resistance and Toxicity” Faced by Oncology Correspond Exactly to the “Efficacy Ceiling and ARIA Safety Risks” Faced by the AD Field
This represents the most fundamental cross-disciplinary insight in this paper and is key to understanding the strategic significance of the AAIC 2026 London Annual Meeting. The reality in oncology: First-generation targeted therapies (monoclonal antibodies, ADCs) have proven their clinical value, but all face the same fate—under the pressure of tumor evolution, a single target will inevitably be circumvented; drug resistance is a matter of time, not probability.At the same time, systemic toxicity (such as bone marrow suppression and interstitial pneumonia) resulting from high-dose ADCs or high-intensity combination regimens constitutes a safety red line that limits their clinical application.
The reality in the AD field: First-generation anti-Aβ monoclonal antibodies have demonstrated the clinical feasibility of “Aβ clearance,” but the efficacy of Aβ clearance alone has nearly reached its ceiling, with limited absolute benefits in cognitive improvement.Furthermore, the incidence of ARIA (cerebral edema, cerebral microbleeds) in ApoE4 carriers has reached levels so high that many clinicians are forced to make difficult trade-offs between efficacy and safety.
Table 1-4: In-Depth Comparison of Current Clinical Pain Points in Oncology vs. AD Neuroscience (Q2 2026)
| Dimension | Current Status in Oncology (Q2 2026) | Current State of AD Neuroscience (Q2 2026) | Common Issues |
| Achievements of First-Generation Drugs | First-generation ADCs (DS-8201) and PD-1 monoclonal antibodies validated the targeted immunotherapy pathway | Anti-Aβ monoclonal antibodies (Leqembi, Kisunla) demonstrated that Aβ clearance can slow cognitive decline | Single-mechanism therapies have proven viable |
| Efficacy Bottlenecks | Drug resistance (secondary progression to PD): approximately 40–60% within 18 months | Efficacy ceiling (CDR-SB difference of approximately 0.45 points): limited clinical impact | Diminishing returns from single-target coverage |
| Safety limitations | ADC toxicity (interstitial pneumonia, myelosuppression); PD-1 immune-related adverse events (irAE) | ARIA-E (cerebral edema)/ARIA-H (cerebral microbleeds) incidence as high as 40%+ in ApoE4 carriers | Safety red lines limit dose escalation |
| Industry responses | Bispecific ADCs, combination with immune microenvironment modulation, upstream silencing with nucleic acid therapeutics | BBB-crossing bispecific antibodies, Aβ/Tau bispecific antibodies, and upstream inhibition of nucleic acid therapeutics (ASO/siRNA) | Collective shift toward multimodal, multi-target, and precision delivery |
| Signals from Industry Conferences | AACR 2026: Bispecific Antibody-Drug Conjugates (ADCs) Are the Hottest Track | AAIC 2026 London Annual Meeting Core Topics: Next-Generation Macromolecular Delivery and Multi-Target Combination Therapies | These two conferences collectively mark the completion of a paradigm shift in the industry |
This table reveals a striking symmetry: oncology and Alzheimer’s disease—two seemingly disparate disease areas—are following nearly identical evolutionary trajectories in 2026, progressing through the stages of “single-molecule dominance → hitting a wall → multidimensional breakthrough.”It is against this historical backdrop that the AAIC London Annual Meeting in July 2026 is destined to be more than just a conventional “annual AD update”; it will become a landmark gathering heralding the entry of neuroscience macromolecular drug R&D into its “refined second half.”
2.0 London Review: Core Technical Topics of the 2026 bio Annual Meeting and the Evolutionary Path of Next-Generation Macromolecules
From July 12–17, the ExCeL Exhibition Center in Docklands, East London, will host the official opening of the AAIC 2026 Annual Meeting.As the world’s largest professional conference on Alzheimer’s disease and neurodegenerative disorders, this year’s London conference is expected to attract over 5,000 registered attendees from more than 80 countries and regions, with over 3,500 research abstracts submitted.The agenda structure of this year’s conference clearly reflects the two core issues currently of greatest concern to the industry: first, how to derive maximum learning value from existing clinical data on first-generation macromolecular monoclonal antibodies (i.e., “Review and Revision”); and second, where the technological evolution of next-generation CNS macromolecular drugs should be directed (i.e., “Breakthroughs and Outlook”).
2.1 “Review and Revision” of Phase III Clinical Data for First-Generation Macromolecular Monoclonal Antibodies
During the official scientific program of the AAIC 2026 London Annual Meeting (July 13–17), multiple Late-Breaking Science presentations from teams at Eisai/Biogen and Eli Lilly will present the latest long-term follow-up data for Leqembi and Kisunla. The significance of these data lies not only in the findings themselves but also in the fact that they will provide a critical “reference framework” for hundreds of biotech companies worldwide that are striving to catch up with the industry leaders.
2.1.1 Latest Phase III Efficacy Follow-Up for Aβ and Tau Monoclonal Antibodies: Changes in the Benefit-to-Risk Ratio for Long-Term Patients Revealed by the Data
Leqembi was approved for marketing in the United States in July 2023, and by July 2026, approximately three years of real-world evidence (RWE) had been accumulated.The long-term follow-up data expected to be presented at AAIC 2026 will address a critical scientific question: following the conclusion of the 18-month Phase III clinical trial, will patients’ cognitive improvement trajectories continue, accelerate, or plateau with continued use of Leqembi?
According to preliminary data from the Leqembi Open-Label Extension (OLE) study published in the *New England Journal of Medicine* (NEJM) in the second half of 2025, among patients who continued treatment after the core trial concluded, the rate of decline in CDR-SB scores showed some “signs of deceleration” between 24 and 36 months——that is, there were statistical signals of a slowing trend in the cognitive decline trajectory among patients who continued treatment. This is encouraging news. However, even in the continuation group, patients’ cognitive function continued to decline over time, albeit at a slower rate—Leqembi has not yet demonstrated the ability to “halt” or “reverse” cognitive decline.
In the realm of tau monoclonal antibodies, Phase III clinical results from several contenders were also a major highlight at this year’s AAIC. The tau-targeting monoclonal antibodies currently furthest along in development include:
① semorinemab (developed by Roche/Genentech, targeting N-terminal tau): The Phase III Tauriel trial in patients with moderate AD has previously released interim data, and full follow-up results are expected to be presented at AAIC 2026.
② Gosuranemab (developed by Biogen, targeting N-terminal tau): A Phase III study is underway in patients with mild cognitive impairment (MCI) to mild AD, and patient enrollment has been completed.
③ Zagotenemab (developed by Eli Lilly, targeting aggregated tau): Primarily targeting patients with moderate AD who already have tau tangles within neurons; Phase III is ongoing.
Table 2-1: Summary of Clinical Progress for Tau-Targeting Monoclonal Antibodies (AAIC 2026 Key Focus List)
| Drug | Target | Developer | Phase III Status | Expected Highlights at AAIC 2026 | Key Challenges |
| semorinemab | N-terminal Tau (monomers + aggregates) | Roche/Genentech | Completed, awaiting final analysis | Complete follow-up data for patients with moderate-stage AD | Weak signal in early-stage clinical trials for mild cases |
| gosuranemab | N-terminal Tau protein | Biogen | Phase III completed | Long-term benefit data for MCI-to-Mild AD | Previous Phase II trial did not meet primary endpoint |
| zagotenemab | Aggregated Tau (fibrils) | Lilly | Phase III ongoing | Interim data unblinded | Doubts regarding the ability of the aggregate-targeting antibody to penetrate the cell membrane |
| JNJ-63733657 | pT217 Phosphorylated Tau | J&J/Janssen | Phase II/III Transition | Data on response to phosphorylated tau markers | Conflict between intravenous dosing frequency and patient compliance |
As shown in the table above, the Tau monoclonal antibody pipeline currently faces the widespread challenge of “limited response in mid-to-late stage patients.” There is a deep scientific rationale behind this: the pathological phosphorylation and aggregation of Tau protein are downstream cascade reactions that occur after the accumulation of Aβ plaques—if intervention to clear Tau is initiated only after the disease has progressed to the stage where Tau tangles have formed extensively, the intervention window may already be closed.This understanding is driving the industry toward a paradigm shift toward “earlier diagnosis (pre-clinical AD stage) combined with dual-target clearance of Aβ and Tau.” This is precisely why the development of ultra-sensitive biomarker detection platforms is of fundamental importance to the entire AD drug R&D landscape.
2.1.2 “Standardized Guidelines” for Safety Risk Control: The Standardization and Upgrading of ARIA Clinical Risk Management
ARIA (Amyloid-Related Imaging Abnormalities) is a common safety challenge for all anti-Aβ monoclonal antibodies currently in development and will undoubtedly be a topic of in-depth discussion at the 2026 AAIC Annual Meeting in London.Understanding the Mechanism Behind ARIA: When anti-Aβ monoclonal antibodies clear Aβ plaques deposited on the walls of brain blood vessels, they trigger a certain degree of localized immune-inflammatory response, leading to a temporary increase in blood-brain barrier permeability and causing cerebral edema (ARIA-E) or microvascular rupture (ARIA-H, manifested as cerebral microbleeds or hemosiderin deposition).
At the AAIC 2026 London Annual Meeting, the Global Alzheimer’s Disease Association ARIA Working Group is expected to officially release the updated Global Consensus Guidelines for the Clinical Management of ARIA (2026 Edition). According to the abstract information released in advance, the core revisions in the new guidelines focus on the following dimensions:
① Standardization of MRI monitoring frequency: For ApoE4 homozygous (ε4/ε4) patients, MRI scans will be required every 8 weeks for the first 6 months, a more frequent schedule than the “every 3 months” recommended in the previous guidelines, to detect ARIA signals earlier.
② Stratified management based on ApoE4 genotype: The guidelines clearly distinguish ARIA risk stratification among ApoE4 homozygotes, heterozygotes (ε4/ε3), and non-carriers, establishing differentiated dosing regimens (including dose adjustments and dosing intervals) for different risk groups.
③ Management standards following an ARIA event: Standardize the criteria for discontinuing treatment after an ARIA occurs, the timing of glucocorticoid intervention, and the dosage and dosing interval for resuming treatment after ARIA resolution.
④ Emergency management protocol for symptomatic ARIA: Provide clinicians with a standardized emergency management pathway for symptomatic ARIA, such as headaches and confusion, including criteria for ICU referral.
Table 2-2: ARIA Risk Stratification and Draft 2026 Monitoring/Dosage Strategy (Compiled based on pre-conference abstracts from AAIC 2026)
| Patient ApoE4 Genotype | ARIA Risk Level | MRI Monitoring Frequency (2026 Draft Guidelines) | Recommended Dosing Strategy | Remarks |
| Non-ApoE4 carriers (ε3/ε3) | Low risk | Months 1–6: Every 3 months; thereafter: Every 6 months | Standard therapeutic dose | May be managed according to standard clinical pathways |
| ApoE4 heterozygotes (ε4/ε3) | Moderate risk | Months 1–6: every 2 months; thereafter: every 3 months | Standard dose; consider dose reduction following ARIA | Risks must be specifically addressed in the informed consent form |
| ApoE4 homozygote (ε4/ε4) | High risk | Months 1–6: Every 8 weeks; thereafter: Every 2 months | It is recommended to start with a low dose and titrate gradually | Some draft guidelines recommend careful evaluation of treatment suitability for this group |
The refinement of the aforementioned ARIA management guidelines holds direct industrial significance for preclinical CXO organizations in the neuroscience field: stricter ARIA monitoring standards imply that the clinical development costs of AD drugs will rise further. This will compel pharmaceutical companies to invest more resources in the preclinical stage—before entering expensive human clinical trials—to predict ARIA risks in animal models. This will generate new demand for preclinical BBB safety assessment services.
2.2 A Strategic Approach: Next-Generation CNS Bispecific Antibodies Drawing on Immuno-ADC Logic
The topic that most excited the global biotech community at the AAIC 2026 London Annual Meeting was not long-term follow-up data on approved drugs, but rather those next-generation technologies still in early clinical or preclinical stages that are rewriting the rules of the game—especially novel CNS bispecific antibodies designed specifically to cross the blood-brain barrier (BBB), drawing on the logic of oncology Immuno-ADCs.
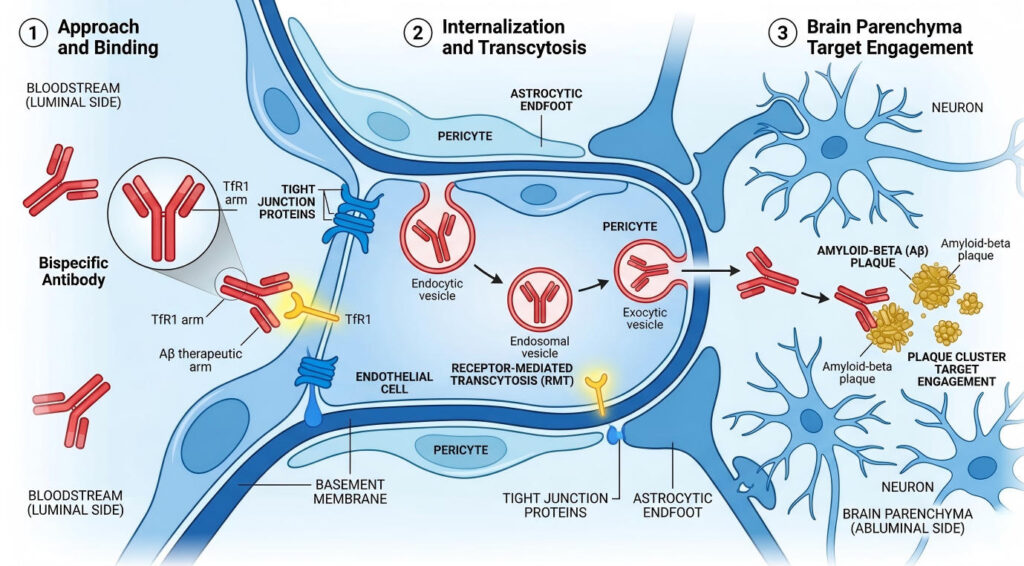
2.2.1 Biomacromolecule Delivery Technology for Crossing the Blood-Brain Barrier (BBB Shuttle): How Transferrin Receptor (TfR)-Mediated Bispecific Antibody Design Achieves “Hundredfold” Brain Delivery
Traditional intravenously administered macromolecular monoclonal antibodies (IgG, molecular weight approximately 150 kDa) face a nearly insurmountable physical barrier: the blood-brain barrier (BBB).Under normal physiological conditions, the tight junctions of endothelial cells, pericytes, and astrocytes in the BBB collectively form a highly selective physical barrier. Only a few specific small molecules can freely cross this barrier, while the vast majority of therapeutic proteins—including monoclonal antibodies—are almost entirely excluded.
The data quantifying this problem are startling: under standard intravenous administration, the efficiency of IgG monoclonal antibodies entering the brain parenchyma is less than 0.1% of the total administered dose. This means that if a patient is injected with 1,000 mg of anti-Aβ monoclonal antibody, the actual amount of drug that reaches the brain and exerts a clearing effect does not exceed 1 mg.The remaining 99.9% remains in the peripheral circulation, which not only wastes resources but is also one of the root causes of ARIA—when large amounts of Aβ are rapidly cleared by high concentrations of monoclonal antibodies in the peripheral circulation, it triggers “Aβ backflow” into the vascular wall, leading to vascular inflammation.
The core concept of BBB Shuttle technology is to utilize the receptor-mediated transcytosis (RMT) mechanism expressed by BBB endothelial cells to “disguise” large-molecule antibodies as “guests” of the BBB endothelial cells, allowing them to cross into the brain via this pathway.Among these, the transferrin receptor (TfR1, also known as CD71)-mediated crossing strategy is currently one of the most extensively studied and rapidly advancing technological pathways globally.
[Industry Background Tip]In 2024, data from a non-human primate study published by Roche in *Science Translational Medicine* showed that an anti-Aβ bispecific antibody designed with a TfR1-mediated BBB shuttle achieved approximately 40–60 times higher drug concentrations in brain parenchyma compared to traditional monovalent monoclonal antibodies, while monoclonal antibody concentrations in peripheral blood were correspondingly reduced by about 70%.This implies: lower systemic exposure and higher effective brain concentrations—thereby significantly reducing the fundamental risk factors for ARIA.
Table 2-3: Summary of Major Global Players in BBB Shuttle Technology (Q2 2026 Perspective)
| Organization | BBB Shuttle Design Approach | TfR Arm Affinity Strategy | Therapeutic Target | Clinical/Preclinical Stage | Key Technology Highlights |
| Roche | TfR1-mediated bispecific antibody (Brain Shuttle™) | pH-dependent low-affinity design | Aβ (anti-Aβ treatment arm) | Phase I (Early-Stage AD) | 40–60-fold increase in intracerebral concentrations in non-human primates; 70% reduction in peripheral Aβ |
| Denali Therapeutics | Transport Vehicle™ (TV) platform | Low-affinity monovalent TfR1 binding domain | Multiple CNS targets (TREM2 agonist, GCase, etc.) | Multiple Phase I/II trials | Highly modular platform with flexible target switching |
| AbbVie (acquired Aliada) | TAPAS™ bispecific platform | Optimized internalization-dissociation kinetics | Tau protein | IND filing stage | The first TfR-mediated bispecific antibody focused on Tau protein clearance |
| JMB (J&J/Merus Collaboration) | BBN bispecific antibody (broad-spectrum LRP1-mediated) | LRP1 receptor (non-TfR) | Aβ/Tau dual-target | Preclinical | Leveraging LRP1’s high natural internalization efficiency |
Interest in BBB Shuttle technology at the 2026 AAIC Annual Meeting will reach a five-year high.The reason is simple: Roche’s Brain Shuttle™ platform is set to release its first Phase I data in humans, marking a milestone for the entire technology pathway at the clinical proof-of-concept (PoC) stage. If Phase I data demonstrate that TfR-mediated bispecific antibodies can indeed achieve higher intracerebral drug exposure in humans while exhibiting lower ARIA incidence and severity compared to conventional monoclonal antibodies, the valuation logic for the entire BBB Shuttle technology ecosystem will be completely rewritten.
2.2.2 Cross-Domain Speculation: How Can the “Synergistic Targeting” Concept of Oncology Bispecific ADCs Be Applied to “Aβ + Tau” Bispecific Antibodies or “Macromolecule + Small Molecule” Innovative CNS Combination Therapy Regimens
If we apply a strict analogy of the oncology “bispecific ADC” concept to the field of AD, what research hypotheses might emerge? The design logic of oncology bispecific ADCs: a single molecule simultaneously blocks two oncogenic targets and carries a chemotherapeutic toxin payload. This triple-pronged attack—synergistic targeting—leaves cancer cells with no escape.
Applied to the field of Alzheimer’s disease, the analogous design is: a single molecule simultaneously clears two pathological proteins (Aβ plaques + hyperphosphorylated Tau) and utilizes a BBB shuttle mechanism for efficient delivery into the brain—this is the so-called “Aβ/Tau bispecific antibody (Bispecific Antibody targeting both Aβ and Tau).” Currently, within academic and biotech circles, this concept has evolved from a “pipe dream”to “active preclinical exploration.”
Another “cross-disciplinary concept” currently sparking heated discussion at AAIC 2026 is the “combination therapy” design involving macromolecular monoclonal antibodies and small-molecule neuroprotective agents. The specific logic is as follows:
① The large-molecule monoclonal antibody is responsible for targeting and clearing pathological proteins (Aβ/Tau), providing the function of “eliminating the enemy”
② Small-molecule neuroprotectants (such as the microtubule stabilizer Epothilone D, GSK-3β inhibitors, and mitochondrial protectants) provide the “survival support” necessary for neuronal survival
③ Ideally, utilizing BBB Shuttle technology, the large-molecule monoclonal antibody “carries” the small-molecule drug to achieve co-delivery—this is conceptually very similar to the “antibody-drug conjugate” (ADC) logic in oncology, except that in the AD field, the “toxin” is replaced by a “protective agent.”
Table 2-4: Summary of Innovative Designs for Next-Generation Multifunctional CNS Macromolecules (AAIC 2026 Perspective)
| Innovative Design | Scientific Logic | Current Maturity | AAIC 2026 Focus | Key Risks |
| Aβ/Tau Bispecific Antibody | Simultaneously blocks Aβ plaques (upstream) and Tau tangles (downstream), covering a broader time window | Preclinical (multiple IND applications in preparation) | ★★★★★ (One of the hottest topics at the annual conference) | Challenges in achieving Kd equilibrium between dual targets; high complexity in macromolecular design and engineering |
| Co-delivery of macromolecules and small molecules to the CNS (ADC-like approach) | Utilizing a BBB shuttle for co-delivery of macromolecular clearance and small-molecule protection for dual efficacy | Early-stage proof of concept (animal model data) | ★★★★ (Emerging topic of discussion) | Complex linker design; significant uncertainty regarding the intracerebral release kinetics of small-molecule neuroprotectants |
| TfR-mediated BBB shuttle + anti-Tau | TfR bispecific antibody carrying an anti-Tau therapeutic arm, enhancing intracerebral exposure of Tau clearance agents | Early-stage clinical trials (AbbVie/Aliada IND phase) | ★★★★ (Extension of the BBB shuttle topic) | Balancing TfR affinity design with iron metabolism safety |
| Trifunctional monoclonal antibody (TriFAb, targeting Aβ+Tau+TfR) | A single molecule with triple functionality: BBB crossing, Aβ clearance, and Tau clearance | Early Concept Exploration (Animal Models) | ★★★ (Cutting-edge academic hypothesis) | Engineering the balance of these three functions is extremely challenging; molecular stability and production complexity are extremely high |
3.0 Cross-disciplinary Exploration at 2026 bio: Potential Intersections of ADCs, Nucleic Acid Therapeutics, and Combination Therapies in Neurodegenerative Diseases

From AACR to AAIC, from oncology to neurodegenerative diseases—the depth of this cross-disciplinary dialogue goes far beyond the simple, independent “transition to multimodal approaches” within each field.An even more exciting possibility lies in the fact that oncology and neuroscience may be converging toward a common technological intersection, where ADCs, nucleic acid therapeutics (RNAi/ASO), and combination therapies of small and large molecules will merge, giving rise to a truly unprecedented therapeutic paradigm. Several key sessions at the AAIC 2026 London Annual Meeting will focus on the latest advances in this cross-disciplinary exploration.
3.1 “ADC-like” Approaches in Alzheimer’s Disease: From Immune Clearance to Precision Targeted Killing/Repair
3.1.1 Concept Transfer: Utilizing Antibody-Drug Conjugate (ADC) Technology to Precisely Deliver Small-Molecule Neuroprotectants to Damaged Neurons
The core logic of Antibody-Drug Conjugates (ADCs) in oncology can be summarized in a single sentence: “The antibody serves as the missile’s guidance system, the small-molecule toxin as the warhead, and the linker as the fuse.” The antibody identifies specific targets on the surface of cancer cells, precisely delivering the entire conjugate to the vicinity of the target cells. The linker is then specifically cleaved within the tumor microenvironment, releasing the toxin warhead to kill the cancer cells.
A group of bold research teams is now posing a reverse question: If the toxin warhead were replaced with a neuroprotective or neuroregenerative agent, could the same “antibody-targeted delivery” logic be used to precisely deliver beneficial small-molecule drugs to damaged neurons, rather than relying on traditional oral or intravenous administration that allows the molecules to circulate indiscriminately throughout the body?
This idea is not far-fetched. The neuroscience community has long grappled with a dilemma: many small-molecule compounds known to possess neuroprotective activity (such as microtubule stabilizers like epothilone D and taxol derivatives,GSK-3β inhibitors, and Nrf2 activators) demonstrate clear neuroprotective effects in cellular and animal models, yet they repeatedly fail in human clinical trials—not because the compounds lack activity, but because the drug concentration actually reaching brain neurons after oral or intravenous administration is far too low. Moreover, the systemic dose required to achieve sufficient brain concentrations would lead to severe peripheral toxicity.
Table 3-1: Summary of promising neuroprotective small-molecule payloads in the CNS “ADC-like” concept (preclinical research perspective, Q2 2026)
| Small-Molecule Payloads | Neuroprotective Mechanism | Challenges with Conventional Administration | Antibody Targets in CNS ADC Design | Current Research Maturity |
| Epothilone D (microtubule stabilizer) | Stabilizes the microtubule cytoskeleton within neurons, antagonizing Tau-induced microtubule depolymerization | High systemic toxicity (similar to Taxol); extremely narrow therapeutic window in the brain | p75NTR (low-affinity neurotrophic factor receptor) | Animal models (AD mice rTg4510) show microtubule restoration; therapeutic window in humans remains to be validated |
| GSK-3β inhibitors (e.g., LY2090314) | Inhibits key kinases involved in Tau hyperphosphorylation, reducing pathological p-Tau production at the upstream level | Low oral bioavailability; poor BBB permeability; rapid hepatic metabolism | TfR1 (using the BBB Shuttle strategy) | Early preclinical stage; being explored in collaboration with Roche Brain Shuttle at select institutions |
| NAD+ precursors (NMN/NR) | Restores neuronal mitochondrial function, improves ATP supply, and delays neuronal apoptosis | Requires extremely high oral doses; limited efficacy with intranasal administration; short half-life in the brain | TREM2 agonist antibody (targeting microglia) | Conceptual stage; currently being explored in conjunction with Denali’s TREM2 agonist platform |
| Sirtuin-1 activators (e.g., SRT1720) | Activates the SIRT1 deacetylase to protect neurons against oxidative stress damage | Highly lipophilic; prone to hepatic metabolism; unstable CNS exposure | EphB2 receptor (highly expressed in hippocampal neurons) | Early-stage concept exploration; no IND-level data available |
Action Recommendations: For CROs and biotech companies monitoring preclinical research opportunities in the CNS space, we recommend closely tracking the poster data from MIT/Stanford at AAIC 2026, as well as the latest developments regarding the expansion of payload types on Denali Therapeutics’ Transport Vehicle platform—these two directions represent the most likely near-term breakthroughs for CNS-targeted ADCs moving from concept to IND.
3.1.2 Industry Frontier Discussion: Feasible Approaches for “Immune Microenvironment Modulators” Targeting Microglia Overactivation in AD
Alzheimer’s disease is essentially a chronic inflammatory disease of the brain—this understanding is not new in the neuroscience community, but over the past five years, as our understanding of the role of microglia in AD pathogenesis has deepened, its implications have been greatly enriched.Microglia are the brain’s resident immune cells, normally responsible for clearing neuronal debris, pathological protein aggregates, and damaged synapses. However, in the pathological environment of AD, the persistent accumulation of Aβ plaques and tau tangles chronically stimulates microglia over the long term, driving them to transform from “protective scavengers” into “destructive killers”——overactivated microglia (M1 pro-inflammatory phenotype) release large amounts of pro-inflammatory cytokines (such as TNF-α, IL-1β, and IL-6) and reactive oxygen species (ROS), which in turn accelerate neuronal apoptosis, creating a vicious cycle.
[Industry Background Tip] Genomic data indicate that loss-of-function variants in TREM2 (such as the R47H mutation) increase the risk of late-onset AD by approximately 2–4 times, comparable to the risk associated with the ApoE4 allele.This finding confirms the causal role of the TREM2 signaling pathway in microglia in AD pathogenesis at the genetic level and provides strong genetic support for the development of TREM2 agonists (Agonistic Anti-TREM2 Antibody).
Table 3-2: Summary of Major Advances in AD Neuroinflammation and Immune Microenvironment Modulation (AAIC 2026 Watch List)
| Target/Strategy | Representative Drugs | Collaborators | Clinical Stage | Scientific Rationale | Highlights of AAIC 2026 |
| TREM2 Agonist Antibody | AL002c | Denali + Biogen | Phase II (INVOKE-2) | Activates the TREM2 pathway in microglia, enhances active phagocytosis of Aβ, and reduces neuroinflammation | Interim data unblinding for INVOKE-2 (PET scans, blood biomarkers) |
| TREM2 agonist antibody | AL002 (another candidate) | Alector + AbbVie | Phase II | Targets different epitopes in the extracellular domain of TREM2 | Comparison with AL002c |
| CSF1R Inhibitor (Microglia Regulation) | Emraclidine | Cerevel (acquired by AbbVie) | Phase II (exploring AD indications) | Modulates microglial activation status to reduce excessive pro-inflammatory responses | Cross-indication (schizophrenia → AD) data on CSF1R modulation |
| Complement system (C1q blockade) | ANX005 (IgG4 anti-C1q) | Annexon Biosciences | Phase II (AD/neurodegenerative) | Inhibits C1q-mediated synaptic elimination, preserving synaptic integrity | Synaptic protection biomarker (NfL levels) data |
| NLRP3 inflammasome inhibitor | MCC950 (and analogs) | Multiple academic/biotech teams | Preclinical → Phase I | Inhibits NLRP3 inflammasome activation in microglia, reducing IL-1β secretion | Preclinical animal model data (Poster presentation) |
This therapeutic area shares structural similarities with the “immune microenvironment modulation” track in oncology, which has already attracted significant attention from certain cross-sector investment firms.Action Recommendation: Preclinical CROs currently evaluating market expansion strategies are advised to carefully assess the strategic value of “neuroinflammation/microglia function assessment” service capabilities. The advancement of clinical trials such as INVOKE-2 is generating outsourcing demand for novel animal models, including validated TREM2 functional activation models and CSF1R modulation models.
3.2 The Rapid Rise of Nucleic Acid Drugs (RNAi/ASO) and Combination Therapies with Small and Large Molecules
If large-molecule monoclonal antibodies are likened to “cleaning up the battlefield downstream” (removing Aβ plaques and Tau tangles that have already accumulated in the brain), then the battlefield for nucleic acid therapeutics lies “upstream”—silencing Tau protein or even the Aβ precursor protein (APP) at the RNA level before they are translated into proteins.
3.2.1 Synergy Between Small and Large Molecules: The Latest Attempts to Use Small Molecules to Modulate Blood-Brain Barrier Permeability and “Clear the Path” for Large-Molecule Monoclonal Antibodies
The inability of large-molecule monoclonal antibodies to enter the brain is one of the most fundamental challenges in AD drug development—as detailed earlier, the BBB Shuttle bispecific antibody technology addresses this issue by “hitching a ride on the TfR1 receptor.”However, another approach focuses on regulating the permeability of the BBB itself: Could a small-molecule drug be used to temporarily and locally “open” the blood-brain barrier, allowing the large-molecule monoclonal antibody to enter the brain, and then restore the BBB to its normal permeability?
“Small-molecule BBB permeability modulators” currently being explored in the academic community include:
① Claudin-5 peptide antagonists: These utilize synthetic competitive peptides to temporarily disrupt the tight junction function of Claudin-5, creating a reversible BBB opening window (lasting approximately 2–6 hours).Experimental data in rodent models have demonstrated a 3- to 5-fold increase in IgG penetration into the brain, but safety assessments for systemic administration in the brain and heart are still ongoing.
② P-gp (P-glycoprotein) efflux pump inhibitors: P-gp is a key active efflux pump on BBB endothelial cells responsible for “pumping” exogenous substances that enter the brain back into the bloodstream. Inhibiting P-gp activity reduces the efficiency of active efflux of macromolecules, thereby indirectly increasing their residence time in the brain.However, P-gp inhibitors have a long history of research, and their systemic effects (drug interactions resulting from P-gp inhibition in the liver and intestines) are known safety concerns.
③ Focused Ultrasound (FUS) combined with microbubble technology: This is currently one of the BBB-opening technologies advancing most rapidly toward clinical translation. By applying focused ultrasound externally to the skull to rupture microbubbles injected into the circulation, the resulting microfluidic effect can create reversible BBB opening in the focal area (lasting approximately 6–24 hours).ExAblate Neuro (developed by InSightec) and SonoCloud (developed by CarThera) have entered the clinical trial phase, and exploratory studies combining these technologies with AD monoclonal antibodies have been initiated at multiple medical centers.
Table 3-3: Summary of Small-Molecule/Physical-Assisted BBB Permeability Enhancement Strategies (Clinical/Preclinical Progress as of Q2 2026)
| BBB Opening Strategies | Technical Principle | Duration of Permeabilization | Clinical Progress | Advantages | Safety Concerns |
| Claudin-5 Peptide Antagonist | Competitively antagonizes tight junctions, reversibly reducing BBB barrier function | 2–6 hours (in vitro/rodent data) | Preclinical (Phase I in preparation) | Pharmacological, systemically controllable, no physical intervention required | CNS safety with long-term repeated dosing is unknown; risk of peripheral BBB opening with systemic administration |
| Focused Ultrasound (FUS) + Microbubbles | Mechanical waves promote microbubble cavitation, resulting in physical, localized BBB opening | 6–24 hours | Phase I/II (exploratory use in combination with lecanemab) | Highly localized; precise and controllable opening of the target area; no systemic effects | Requires specialized equipment; consistency of ultrasound transmission through the skull varies significantly among patients |
| P-gp efflux pump inhibitor | Inhibits BBB endothelial efflux pumps, reducing active drug efflux | Administered concurrently with drug delivery (transient inhibition) | Preclinical (with a body of historical research) | Can be administered orally; simple logic for co-administration with large-molecule monoclonal antibodies | Systemic P-gp inhibition leads to drug interactions; risk of hepatotoxicity |
| MMP activators (temporary BBB remodeling) | Activate matrix metalloproteinases to locally degrade BBB structural proteins | Minutes to hours | Early-stage concept exploration | Significant localized effects | Risk of uncontrolled localized neuroinflammation; difficult to precisely control in vivo |
Among these, focused ultrasound (FUS) technology is currently the most noteworthy approach for BBB opening at AAIC 2026, as clinical exploration of its combination with lecanemab has already yielded early-stage human data.Two teams from West Virginia University and Columbia University are expected to present Phase I safety data at the annual meeting on the combination of FUS and lecanemab in early-stage AD patients—including comparisons of Aβ clearance efficiency and ARIA incidence in localized BBB-open regions. This will be among the first human data to formally demonstrate the “combination” of physical BBB-opening technology with first-generation AD monoclonal antibodies.
3.2.2 Nucleic Acid Therapeutics (ASO/RNAi) as a Strategic Complement to Upstream Inhibition of Tau Protein Expression by Monoclonal Antibodies: The Ultimate Potential for Future Combination Therapies
The field of nucleic acid therapeutics has experienced a simultaneous surge in both basic research and clinical applications in recent years. Among its two primary technological branches—antisense oligonucleotides (ASO) and RNA interference (RNAi, including siRNA and shRNA)—milestone clinical breakthroughs have been achieved in the fields of neuroscience and liver diseases, respectively.
BIIB080 (formerly known as ION338), developed by Ionis Pharmaceuticals, is an ASO drug that targets the mRNA of the MAPT gene (which encodes the Tau protein). Administered via intrathecal injection, it is designed to silence Tau protein production.Phase I data published in 2023 showed that BIIB080 successfully reduced Tau protein levels in cerebrospinal fluid by approximately 50–70% in patients with mild AD, with acceptable tolerability. This marks the first time in human history that a nucleic acid drug has achieved a measurable reduction in Tau protein levels in the brains of AD patients—a milestone that will be further validated by clinical data at AAIC 2026.
Table 3-4: Summary of Clinical Progress for CNS Nucleic Acid Drugs (ASO/RNAi) (Focusing on Upstream Targets of Tau and Aβ, Q2 2026)
| Drug | Type | Target Gene/RNA | Company | Clinical Stage | Key Data | Route of administration |
| BIIB080 (ION338) | ASO (antisense oligonucleotide) | MAPT mRNA (Tau protein mRNA) | Ionis + Biogen | Phase I/II (ATLAS Trial) | 50–70% reduction in cerebrospinal fluid Tau (Phase I) | Intrathecal injection |
| JNJ-0049 (ASO) | ASO | MAPT mRNA | J&J/Janssen + Ionis | Phase II | Phase I (detailed data not disclosed) | Intrathecal injection |
| QR-1123 (siRNA) | RNAi (siRNA) | APP mRNA (Aβ precursor protein) | ProQR/miRagen | Preclinical → Phase I Preparation | Targeting APP Swedish mutation-associated familial AD | Intracranial/intraventricular |
| VY-HTT01 (RNAi) | AAV vector RNAi | HTT mRNA (Huntington’s disease) | Voyager/Novartis | Phase I/II | 60%+ reduction in HTT protein levels in vivo | Stereotactic intracerebral injection |
Currently, the question most exciting the industry is: Can the combination of ASOs and large-molecule monoclonal antibodies produce synergistic effects that surpass those achieved by either agent alone? Theoretically, the logic behind this combination is extremely clear:
① Large-molecule monoclonal antibodies (such as Leqembi) are responsible for clearing existing Aβ plaques in the brain—downstream clearance, handling “existing waste”
② ASOs (such as BIIB080) are responsible for preventing the production of new Tau proteins at the RNA level—upstream inhibition, shutting down the “garbage factory”
③ In theory, the combination can simultaneously reduce the stock of Aβ plaques (via antibody clearance) and the accumulation of Tau tangles (via ASO inhibition), attacking two key pathological mechanisms at once to produce a true “1+1>2” synergistic effect.
[Industry Background Tip] Preclinical studies in mouse and non-human primate models have already demonstrated that the combination of Aβ-clearing monoclonal antibodies and MAPT ASOs outperforms either monotherapy in terms of cognitive function preservation and neuronal survival.However, the greatest challenge in advancing this combination strategy to human clinical trials is the differing administration routes of the two drugs (monoclonal antibodies via intravenous injection, ASOs via intrathecal injection)—the concurrent use of these two highly invasive administration methods will significantly increase patient compliance challenges and clinical operational complexity.
Action Recommendation: For CROs focused on the AD pipeline, the evaluation of CNS delivery efficiency for nucleic acid therapeutics and the development of pharmacodynamic models for combination therapy will become emerging service demands from the second half of 2026 through 2027.Recommendation for Early Planning: Establish a validated quantitative model for MAPT ASO silencing efficiency and a pharmacodynamic evaluation platform for “ASO + monoclonal antibody” combination therapy to capture preclinical outsourcing needs from the first wave of AD pharmaceutical companies entering clinical exploration of combination therapy.
4.0 Attending 2026 bio: How Participants Can Maximize the “Upstream and Downstream Support” Traffic Peak at AAIC

The AAIC 2026 London Annual Meeting is not merely a collection of academic presentations; it is also the most significant annual commercial gathering for the global neuroscience industry’s upstream and downstream sectors. In the official exhibition area at the ExCeL Exhibition Center, hundreds of exhibitors will showcase the latest products and services spanning diagnostic platforms, clinical trial services, digital patient follow-up tools, and neuroimaging solutions.For attendees in various roles—R&D scientists, clinicians, business development specialists, investors, and heads of CXO service firms—determining the most effective allocation of time and energy across the five-day intensive conference schedule is a practical challenge that warrants careful planning.
4.1 The Cross-Disciplinary Convergence of Diagnostics and R&D: The Strategic Significance of Ultra-Sensitive Biomarker Platforms
4.1.1 Why Does the Development of Large-Molecule Drugs Rely Heavily on Ultra-Sensitive Detection? Taking Ultra-Sensitive Large-Molecule Detection Platforms Such as Quanterix and Fujirebio as Examples
Prior to the emergence of Quanterix’s Simoa technology and Fujirebio’s Lumipulse platform, the “gold standard” approach for diagnosing Alzheimer’s disease required one of the following two methods:
① PET brain scan (Amyloid PET or Tau PET): A radiolabeled Aβ-specific ligand (such as Florbetapir, Florbetaben, or Flutemetamol) is administered intravenously to the patient, followed by positron emission tomography (PET) to visualize Aβ deposits in the brain.This is the most direct way to confirm AD pathology, but a single scan costs approximately $3,000–5,000 in the U.S. healthcare system and requires access to PET scanners, making it virtually impossible to implement in most countries and regions worldwide.
② Lumbar Puncture: Cerebrospinal fluid (CSF) is extracted via lumbar puncture to measure the Aβ42/Aβ40 ratio and AD marker proteins such as p-Tau181.AD biomarkers are present at high concentrations in CSF, allowing for highly accurate detection. However, lumbar puncture is an invasive procedure with certain risks (such as post-operative headaches and infection), and patient acceptance is low. Compliance with repeat testing (for efficacy follow-up) is extremely poor.
The common issues with these two methods are that they are expensive, difficult to perform, and frequent follow-ups are impractical—this directly leads to extremely costly and time-consuming “patient screening” in AD clinical trials, resulting in severe delays in patient recruitment for multiple large-scale Phase III clinical trials worldwide.
Now, ultra-sensitive detection platforms, represented by Quanterix’s Simoa (Single Molecule Array) technology, are completely disrupting this landscape.The core innovation of Simoa technology lies in increasing the detection sensitivity of traditional ELISA by approximately 1,000 to 10,000 times, enabling the detection of AD-related proteins in blood at extremely low concentrations (in the femtogram per milliliter range, fg/mL), including pTau-217, pTau-181,GFAP (glial fibrillary acidic protein), and NfL (neurofilament light chain).
Table 4-1: Comparison of Major Technical Approaches and Products for Ultra-Sensitive AD Biomarker Detection Platforms (Q2 2026)
| Assay Technology | Representative Companies/Products | Sensitivity Range | Target Biomarker | Application Scenarios | Current Regulatory Status (U.S.) |
| Simoa (Single-Molecule Array) | Quanterix Simoa HD-X | Femtograms per milliliter (fg/mL) | pTau-217, pTau-181, NfL, GFAP, Aβ42/40 ratio | Preclinical studies, Phase I/II pharmacokinetic monitoring, research-grade testing | LDT (Laboratory-Developed Test), partially designated as a Breakthrough Device by the FDA |
| CLEIA (Chemiluminescent Enzyme Immunoassay) | Fujirebio Lumipulse | Pico-grams per milliliter (pg/mL) sensitivity (superior to traditional ELISA) | CSF Aβ42/Aβ40, p-Tau181, Total Tau | CSF testing (clinical diagnosis, clinical trial enrollment screening) | CE Certified (EU); FDA PMA application in progress |
| Mass spectrometry (LC-MS/MS) | C2N Diagnostics PrecivityAD2 | pg/mL range (blood mass spectrometry) | Plasma Aβ42/40 ratio (precise mass spectrometry quantification) | Clinical diagnostics (patient-specific testing), clinical trial enrollment | LDT (C2N in-house laboratory), FDA approval pending |
| Electrochemiluminescence (ECL) | Roche Elecsys pTau217 | pg/mL range | Plasma pTau-217 | Clinical diagnosis (point-of-care testing available at pharmacies/clinics) | FDA-approved (approved in 2024 for the diagnosis of AD) |
As shown in the table above, blood biomarker testing technology is rapidly evolving from a “research tool” into a “clinical diagnostic tool.” This will make large-scale Phase 3 clinical trials for AD—previously affordable only to mega-pharmaceutical companies—feasible for mid-sized biotech firms. This is an ongoing process of industry democratization, and the AAIC 2026 Annual Meeting in London will serve as a pivotal milestone for the industry to publicly acknowledge and advance this process on a large scale.
4.1.2 Hidden Business Opportunities in Preclinical CXO and Pharmaceutical Outsourcing: How the Widespread Adoption of Blood Biomarker Testing Will Radically Transform Clinical Screening and Patient Stratification for AD
The widespread adoption of blood biomarker technology has not only transformed the cost structure of clinical diagnosis and drug development for Alzheimer’s disease (AD), but has also directly opened up a new market for CXO outsourcing services—AD biomarker testing—a niche segment that was virtually nonexistent in the past.
The combination of blood biomarker screening and ultra-sensitive CRO outsourcing platforms is creating an entirely new patient screening pathway:
① Primary care physicians in community clinics or neurologists can collect blood samples from patients with suspected early-stage cognitive impairment and send them to CRO-partnered laboratories for pTau-217 or Aβ42/40 ratio testing.
② The CRO laboratory issues a standardized, validated biomarker report (identifying patients with a high probability of positivity) and provides it as “pre-screening results” to the pharmaceutical company’s clinical trial team.
③ Patients with a high probability of positivity then undergo PET confirmation (a “two-step” screening strategy), significantly reducing the number of unnecessary PET scans and saving clinical trial costs.
④ As a result, the pharmaceutical company’s clinical trial enrollment efficiency increases by 3–5 times, while the AD pathological positivity rate (true positive rate) among enrolled patients also improves significantly due to prescreening.
Table 4-2: Cost/Efficiency Comparison of Different Enrollment Screening Strategies for AD Clinical Trials (Q2 2026)
| Screening Strategy | Estimated Cost per Patient for Screening | Screening Cycle | Aβ-Positive Patient Detection Rate | Applicable Scenarios |
| Conventional PET Scan (Single-Step Strategy) | $3,000–5,000 per person | 2–6 weeks (waiting time + image interpretation) | Approx. 40–50% (general memory clinic population) | Large academic medical centers, well-funded multinational pharmaceutical companies conducting Phase III trials |
| Blood biomarker (pTau-217) prescreening + PET confirmation (two-step strategy) | $500–800 (blood test) + $3,000–5,000 (PET scan, though numbers have decreased significantly) | 1–3 weeks (blood) + 2–6 weeks (PET, limited to high-risk individuals) | Overall screening efficiency increased by 3–5 times; PET usage reduced by 70%+ | Mid-sized biotech Phase III trial; large-scale screening project in early stages |
| Pure blood biomarker screening (Phase I/II exploratory studies) | $300–600 per person | 3–7 days | Depending on cutoff settings, false positive rate is approximately 10–20% | Early-stage clinical Phase I/II; proof-of-concept; large-scale epidemiological studies |
| Cerebrospinal Fluid (CSF) Puncture Screening | $1,000–2,000 per person (including procedure) | 2–4 weeks | Approximately 60–70% (outpatients with memory impairment) | Pharmacodynamic studies requiring high-precision CSF data; Early Phase I |
For preclinical CROs, the widespread adoption of blood biomarkers presents a direct opportunity: establishing standardized service capabilities for “blood AD biomarker testing in animal models.“In preclinical animal studies of AD (AD mouse models such as APP/PS1, 5xFAD, and 3xTg-AD), assessing the pharmacodynamic effects of drug candidates by measuring biomarkers such as pTau, NfL, and GFAP in peripheral blood is a preclinical pharmacodynamic evaluation method that is increasingly recognized by pharmaceutical clients.Action Recommendation: CROs focusing on the AD sector are advised to proactively explore collaboration plans with the Quanterix Simoa platform and review Roche’s promotion policies for the Elecsys platform within academic and CRO institutions, to assess the feasibility and strategic value of incorporating “standardized preclinical AD blood biomarker testing” capabilities into their service portfolios.
4.2 High-Value Fundraising/Collaboration Guide for the London ExCeL Venue
4.2.1 For R&D Professionals: Focus on Specific Academic Posters and Educational Workshops to Capture Unpublished BBB Delivery Data
Given the structure of the AAIC 2026 scientific program, the most valuable content for R&D professionals prioritizing “first-hand information” is often not found in the plenary lectures in the main hall, but rather in the following easily overlooked corners:
Pre-Conference Workshops (July 10–11) Two days before the official conference opens, AAIC typically organizes a series of small-scale, specialized educational workshops, each limited to 50–150 participants, focusing on in-depth discussions of specific technical topics. High-value pre-conference workshop topics expected at the 2026 London conference (based on the published draft agenda) include:
① “Blood-Based Biomarker Standardization Workshop”: Technical experts from Quanterix, Roche, Fujirebio, and C2N Diagnostics will participate to discuss comparability and interoperability standards for pTau-217/Aβ42/40 test results across different platforms.This is one of the most pressing technical challenges currently facing the field of AD blood testing; participants will gain access to previously unpublished cross-platform comparison data.
② “BBB Drug Delivery Technology Workshop”: This session will feature the latest animal study data from Denali, Roche, AbbVie/Aliada, Lundbeck, and other organizations on TfR-mediated bispecific antibodies and LRP1-mediated delivery.This is one of the sessions with the “highest density of unpublished data” at the 2026 AAIC; all R&D professionals interested in the BBB delivery field are advised to register in advance.
Table 4-3: Guide to Finding Key Posters for R&D Professionals at the AAIC 2026 London Annual Meeting
| Poster Category | Keyword Search Recommendations | Key Institutions to Watch | Data Value | Interaction Recommendations |
| BBB Shuttle Intracerebral Delivery Efficiency | “TfR-mediated”, “Brain Shuttle”, “BBB penetrance” | Roche/Genentech, Denali, AbbVie/Aliada | First-in-human Phase I PK/PD data (some not yet formally published) | Focus on CSF drug concentration data; inquire about ARIA incidence compared to conventional monoclonal antibodies |
| Validation of ultra-sensitive blood biomarker performance | “pTau-217 cutoff”, “plasma biomarker”, “cross-platform” | Quanterix, Fujirebio, C2N, AIBL/ADNI datasets | Real-world triangulation data comparing blood, CSF, and PET | Inquire whether the pTau-217 cutoff in Asian populations is consistent with that in Caucasian populations |
| Preclinical Aβ/Tau bispecific antibody | “bispecific”, “Aβ and Tau”, “dual targeting” | MIT, Stanford, ETH Zurich, UCB | Latest cognitive improvement data in in vivo AD mouse models | In-depth understanding of linker design and in vivo dual-target binding kinetics |
| TREM2 agonist biomarker data | “TREM2 agonist”, “microglial activation” | Denali (AL002c INVOKE-2), Alector | Latest interim cohort data from INVOKE-2 (PET + blood biomarkers) | Inquire about data on microglial activation status vs. neuroinflammatory balance following TREM2 agonist administration |
| New Technologies for CNS Nucleic Acid Drug Delivery | “ASO CNS delivery”, “intrathecal”, “MAPT” | Ionis, Biogen, and the Boston Children’s Hospital CNS team | Latest interim data from the ATLAS Phase II trial of BIIB080 (Tau ASO) | Focus on optimizing the frequency of intrathecal injections (studies on reducing frequency from monthly to quarterly) |
4.2.2 For BD and Investors: How to Use Booth Distribution to Infer Multinational Pharmaceutical Companies’ (M&A) Upcoming “Shopping Spree” Preferences in the Neuroscience Field
For attendees from business development (BD) and investment firms, the greatest value of the AAIC 2026 London Annual Meeting lies in an irreplaceable intelligence opportunity: observing, within the same physical space, which startup biotech booths the BD teams of the world’s top multinational pharmaceutical companies are visiting. Below is a practical strategy for gathering “reverse M&A intelligence”:
① Observe Booth Dwell Time: In the Exhibition Hall, BD teams from major pharmaceutical companies typically appear in groups of 2–3 people and carry no identification other than their conference badges. If they linger at a biotech startup or academic spin-off booth for more than 20 minutes, it often indicates concrete interest.Key Focus Areas: Biotech booths specializing in “TfR-mediated BBB shuttling technology”; academic spin-off biotechs focused on “Aβ/Tau bispecific antibodies” (typically clustered in the exhibition’s “Innovation Theater” area); and diagnostic technology companies with mature, ultra-sensitive biomarker platforms that are expanding into CRO and clinical trial support services.
② Capturing “Satellite Symposium” Signals: During AAIC, numerous multinational pharmaceutical companies and biotech firms hold private “satellite symposia” or “closed-door business development meetings” at luxury hotels in the London area (such as The Biltmore Mayfair and the InterContinental London Park Lane). It is recommended to use industry networks to inquire in advance about the dates and topics of these satellite symposia and actively seek invitations to attend.
③ Analysis of Booth Size and Location: In the AAIC exhibition layout, booth location and size often reflect an exhibitor’s strategic priorities. We recommend that BD professionals quickly scan the main exhibition layout during the opening exhibition on July 13, the first day of the annual conference, and compile a list of startup exhibitors that are “well-located, have thoughtfully designed booths, but are not yet widely known.”
Table 4-4: AAIC 2026 London Annual Conference BD M&A Intelligence Guide—High-Priority Target Characteristics and Potential Buyer Matches
| M&A Target Characteristics | High-Priority Booth Characteristics | Core Technology Tags | Potential Buyers (Major Players) | 2026 H2 M&A Probability Assessment |
| Highly Efficient BBB Shuttling Technology | Booth highlights drug concentration data in non-human primate brains; demonstration centers on the “dose-brain exposure” relationship | TfR-mediated bispecific antibodies, LRP1-mediated delivery, and synergistic combination with FUS | Roche, Eli Lilly, Eisai, AbbVie, Lundbeck | ★★★★★ (Highest demand; major companies prioritize building BBB delivery capabilities) |
| Aβ/Tau Bispecific Antibody Platform | Excellent preclinical cognitive data in AD mice; data on CSF dual-target neutralization efficiency | Bispecific antibody design, aggregate clearance efficiency | Roche/Genentech, Eisai, BMS, Eli Lilly | ★★★★ (Clear market potential; multiple major pharmaceutical companies are pursuing this direction) |
| Highly Sensitive AD Blood Diagnostic Platform | Booth features multicenter real-world blood biomarker data; already FDA-approved or CE-marked | pTau-217/Aβ42/40, ultra-sensitive ECL or Simoa | Roche Diagnostics, BioMérieux, Siemens Healthineers | ★★★★ (High value in the “diagnostics + therapeutics” integrated business model) |
| Optimization of CNS nucleic acid drug delivery | Data on cerebrospinal fluid distribution; optimized dosing frequency (from monthly to quarterly) | LNP-encapsulated ASO, PEGylation optimization, neuron-targeted ASO delivery | Ionis (licensed), Novartis, BioNTech | ★★★ (Low technological maturity, late M&A window) |
| TREM2 agonist platform (non-AL002c) | Data on TREM2 epitopes differentiated from Denali/Alector; preclinical data demonstrating dual effects of reduced neuroinflammation and Aβ clearance | Differentiated TREM2 agonism, activation of microglial function | J&J, Merck, Eli Lilly (AD immunotherapy portfolio) | ★★★ (Relies on INVOKE-2 clinical data readout as a catalyst) |
5.0 Summary and Outlook: Investment and R&D Trends in the Global CNS Sector After 2026 bio
After an in-depth review of the first four chapters, we have established a comprehensive understanding of the AAIC 2026 London Annual Meeting from multiple perspectives. Now, let us take a step back from this “London review” to distill the most strategic themes worth pursuing in the global neuroscience (CNS) sector in the second half of 2026.
5.1 From “Effective Treatment” to “Safety, Precision, and Multi-Targeted Approaches”: A Paradigm Shift in AD Drug Development
If we were to summarize the shift in global Alzheimer’s disease drug R&D thinking following the AAIC 2026 London Annual Meeting in a single sentence, it would be this: “Proving that a treatment works is no longer enough.”
The successes of Leqembi and Kisunla have resolved the question of “whether treatment is possible.” The core focus of the AAIC 2026 London Annual Meeting has now collectively shifted to “how to treat patients more safely, precisely, and sustainably.” This paradigm shift encompasses profound changes across at least the following three dimensions:
① Safety-First Design: The high incidence of ARIA (particularly among ApoE4 carriers) has become a fundamental challenge that AD macromolecular drug developers must address at the molecular design level—not merely through clinical management. The essence of BBB Shuttle technology is to achieve higher intracerebral concentrations with lower peripheral blood concentrations, thereby reducing the underlying basis for ARIA at its source.
② Precision CNS Delivery: The 0.1% BBB penetration rate of traditional large-molecule monoclonal antibodies has become an unacceptable engineering flaw by 2026.TfR-mediated bispecific antibody delivery, LRP1-mediated transport technology, and focused ultrasound BBB-opening technology represent three precision delivery approaches rapidly advancing from preclinical to clinical stages. By 2027, “designing for BBB permeability from the outset” will evolve from a patent advantage held by advanced biotech companies into a basic entry requirement for the field.
③ Multi-target Combination: Both single-target Aβ clearance and single-target Tau silencing have demonstrated clear limitations in efficacy. Aβ/Tau bispecific antibodies and combination regimens of macromolecules and nucleic acid therapeutics are emerging as the mainstream technological direction for next-generation AD treatments.The logic behind these combinations—”upstream inhibition + downstream clearance”—will begin human clinical trials in the second half of 2026.
Table 5-1: Comparison of Core Dimensions in the Paradigm Shift of AD Drug R&D (2025 vs. Post-2026)
| Paradigm Dimension | Mainstream Approach (2023–2025) | Shift in Direction Starting in 2026 | Technological Platform |
| Efficacy Goals | Slowing Cognitive Decline | Stopping/reversing | Dual-target clearance of Aβ and Tau; upstream silencing via ASO |
| Safety Design | Post-market surveillance + clinical management (ARIA post-market surveillance) | Safety-first molecular design to reduce ARIA incidence | BBB Shuttle (reducing peripheral Aβ clearance rate); low-dose initiation strategy |
| Delivery Method | Intravenous injection of standard IgG (BBB permeability <0.1%) | Receptor-mediated delivery (10–100-fold increase in BBB permeability) | TfR-mediated bispecific antibodies; LRP1-mediated fusion proteins; FUS-assisted delivery |
| Timing of treatment | Patients with early-stage/mild AD (already exhibiting clinical symptoms) | Pre-symptomatic screening + preventive intervention | Early screening using highly sensitive blood biomarkers; cohort studies in high-risk populations (ApoE4 carriers) |
| Drug type | Monoclonal Antibodies (Biologics) | Multimodal: Combination of macromolecules + nucleic acid therapeutics + small molecules | ASO/siRNA upstream silencing + monoclonal antibody downstream clearance + small-molecule neuroprotection |
The significance of this paradigm shift lies not in a single technological breakthrough, but in a systematic strategic restructuring—from molecular design and delivery engineering to clinical trial design, every aspect of AD drug R&D is being re-examined and rewritten.
5.2 Following the 2026 London Summit, which biotech startups possessing “multimodal/cross-disciplinary technologies” will be more likely to secure contracts from multinational pharmaceutical companies?
Following the conclusion of the AAIC 2026 London Annual Meeting, the global neuroscience investment and financing market in the second half of 2026 will use its outcomes as a new pricing benchmark. The following is a systematic forecast of the profile of biotech startups “most likely to secure contracts from major multinational companies or achieve M&A premiums.”
Key Requirement: Possession of a “core technology platform” that can be directly integrated by major companies, rather than merely a single product pipeline. The logic behind this round of industry M&A has shifted from “buying products” to “buying platforms.”What interests major companies is not “whether you have a Phase II bispecific antibody candidate,” but rather “whether your bispecific engineering platform is versatile enough to incorporate my Tau target within 6–12 months and generate a new candidate.”
Table 5-2: Profile of the Most Promising Neuroscience Biotech Companies and Projected Premium Valuations Following the 2026 AAIC in the Second Half of the Year
| Biotech Profile | Core Technology Elements | Potential Major Buyers | Valuation Catalysts Post-AAIC 2026 | Probability of Premium Valuation |
| Companies with High-Efficiency BBB Shuttling Technology Platforms | Owns IP for TfR/LRP1-mediated delivery platforms; possesses in vivo drug concentration data in non-human primates; has Phase I safety data (human) | Roche, Eli Lilly, Eisai, AbbVie | Positive Phase I data from Roche Brain Shuttle → Sector valuation re-rating | ★★★★★ |
| Pioneer in Aβ/Tau bispecific antibodies | Resolved the issue of affinity balance between dual targets; has cognitive improvement data in AD mice; has data showing reduction in dual CSF biomarkers | Roche/Genentech, BMS, Eli Lilly | AAIC 2026 Poster Data Released → First IND Approved | ★★★★ |
| Highly Sensitive AD Blood Biomarker Platform Company | Offers FDA-approved/CE-marked blood AD biomarker products; maintains a multicenter real-world database | Roche Diagnostics, Siemens, Abbott | The FDA requires that clinical trials for AD drugs must include blood biomarker companion diagnostics → Market expansion | ★★★★ |
| Companies specializing in high-efficiency delivery technologies for CNS nucleic acid therapeutics | Possesses CNS-specific LNP or neuron-targeting ASO delivery platforms; BBB permeability increased by more than 10-fold compared to baseline | Ionis (licensed), Novartis, BioNTech | Positive Phase II data for BIIB080 ATLAS → Overall momentum in the Tau ASO space | ★★★ |
| TREM2/Microglia Function Modulation Platform | Differentiated TREM2 agonist data (distinct from AL002c); animal data demonstrating dual effects of reduced neuroinflammation and Aβ clearance | J&J, AbbVie, Eli Lilly | INVOKE-2 Phase II data unblinding → Clinical validation of the TREM2 target | ★★★ |
| AD Preclinical CRO/Research Tool Provider (Upgraded Version) | Established outsourcing capabilities for blood biomarker testing + multiple validated AD animal models (including efficacy evaluation of ASO + monoclonal antibody combination therapy); serving Phase I/II AD clinical teams | Eli Lilly, Eisai, and small-to-medium-sized AD biotech companies (preclinical research outsourcing) | Increased regulatory requirements for blood biomarkers → Surge in demand for outsourcing to CROs | ★★★ (Service outsourcing, not an M&A target) |
Looking at the six profiles in the table above, one common characteristic runs through them all: possessing “multi-modal technology portfolio capabilities.“Monoclonal antibodies targeting a single target, no matter how strong the data, will struggle to command a premium valuation in the 2026 M&A market; conversely, biotech companies holding the “trinity” of “high-efficiency BBB crossing + dual-target clearance + ultra-sensitive biomarker validation” are becoming the most sought-after names on major pharmaceutical companies’ acquisition lists.
This trend aligns perfectly with the logic of the oncology M&A market at AACR 2026: oncology biotech companies possessing combination capabilities such as “PD-1/VEGF bispecific antibodies + ADCs” or “bispecific antibody ADCs + immune microenvironment modulation” commanded significantly higher average premiums in M&A valuations during Q1/Q2 of 2026 compared to companies with only single-target products.
This gathering in London in July 2026 is more than just the annual feast of neuroscience. It is a collective declaration of the global biopharmaceutical industry’s paradigm shift from “going it alone” to “joint operations.” Those who understand the significance of this gathering will make decisions between the second half of 2026 and 2027 that will alter the trajectory of their careers.
6.0 2026 bio: Frequently Asked Questions (FAQ)

The following 5 frequently asked questions should be translated into English and uploaded together to increase visibility in Google’s “People also ask” search results.
Q: What are the main dates and venue for the AAIC 2026 Annual Meeting in London?
A: The AAIC 2026 Annual Conference will be held from July 12–17, 2026, at the London ExCeL Exhibition Centre in Docklands, East London. Pre-Conference Workshops will take place on July 10–11, offering researchers one of the best opportunities to access the latest unpublished data.The official Scientific Programme runs from July 13–17, with the main exhibition area open concurrently. The conference is expected to attract over 5,000 registered attendees from more than 80 countries and regions, with over 3,500 research abstracts submitted, making it one of the world’s largest and most influential professional conferences on Alzheimer’s disease and neurodegenerative diseases.
Q: What is ARIA? What risks should patients be aware of when receiving AD monoclonal antibody therapy?
A: ARIA (Amyloid-Related Imaging Abnormalities) is the primary safety concern associated with treatment using anti-Aβ monoclonal antibodies (such as Leqembi and Kisunla). It is classified into two types:
① ARIA-E (edema): Local immune reactions triggered by the antibody’s clearance of Aβ lead to a temporary increase in blood-brain barrier permeability, resulting in fluid accumulation in brain tissue. The incidence rate among Leqembi users is approximately 12.6%.
② ARIA-H (Hemorrhagic): Localized vascular inflammation causes microvascular rupture, manifesting as cerebral microbleeds or hemosiderin deposits. The incidence rate is approximately 17.3% among Leqembi users and as high as 31.4% among Kisunla users.
Key risk factors: The ApoE4 genotype is the most significant genetic risk factor for ARIA—the incidence of ARIA in ApoE4 homozygotes (ε4/ε4) is 3–4 times higher than in non-carriers.The updated Global Consensus Guidelines for ARIA Management (2026 Edition) will be released at the AAIC 2026 Annual Meeting in London, establishing differentiated MRI monitoring frequencies and dosing strategies for patients with different ApoE4 genotypes. Patients should undergo ApoE4 genotyping and baseline MRI scans prior to treatment and strictly adhere to the prescribed MRI monitoring schedule during treatment.
Q: What is BBB Shuttle technology, and how does it help overcome the challenge of drug delivery across the blood-brain barrier?
A: BBB Shuttle technology is a novel drug delivery platform specifically developed to address the inability of large-molecule drugs (such as monoclonal antibodies) to effectively cross the blood-brain barrier (BBB). Its core principle is as follows:
Under normal physiological conditions, the efficiency of IgG monoclonal antibodies (with a molecular weight of approximately 150 kDa) entering the brain is less than 0.1% of the total administered dose—meaning that 99.9% of the injected dose remains in the peripheral blood. This is not only wasteful but also one of the root causes of ARIA (amyloid-related imaging abnormalities).
The design concept behind BBB Shuttle technology is to engineer monoclonal antibodies as “bispecific antibodies”——one “arm” recognizes receptors on BBB endothelial cells (most commonly the transferrin receptor TfR1/CD71) and, by leveraging the endothelial cells’ natural “receptor-mediated transport (RMT)” mechanism, “hitchhikes” across to the brain side; the other “arm” performs therapeutic functions, such as clearing Aβ plaques or tau tangles.
Representative platforms include Roche’s Brain Shuttle™ platform (which achieved a 40- to 60-fold increase in intracerebral drug concentrations in non-human primate studies), Denali Therapeutics’ Transport Vehicle™ (TV) platform, and AbbVie/Aliada’s TAPAS™ platform.At the AAIC 2026 London Annual Meeting, the first human Phase I data from Roche’s Brain Shuttle will be the most closely watched clinical proof-of-concept milestone for the entire technology pathway.
Q: What are TREM2 agonists? What role do they play in the treatment of Alzheimer’s disease?
A: TREM2 (Triggering Receptor Expressed on Myeloid cells 2) is a receptor protein expressed on the surface of brain microglia.Genomic studies have found that loss-of-function variants of TREM2 (such as the R47H mutation) increase the risk of late-onset AD by approximately 2–4 times in carriers—confirming, at the genetic level, the causal role of the TREM2 signaling pathway in AD pathogenesis.
TREM2 agonist antibodies (such as AL002c, jointly developed by Denali and Biogen) work by activating the TREM2 signaling pathway in microglia, prompting these “brain scavengers”to switch from a pro-inflammatory state (M1 phenotype) back to a protective state (M2 phenotype), enhancing their ability to actively phagocytose Aβ plaques while reducing the release of pro-inflammatory cytokines (TNF-α, IL-1β), thereby breaking the vicious cycle of “Aβ accumulation → excessive microglial activation → increased neuroinflammation → neuronal apoptosis.”
Interim data from the INVOKE-2 (Phase II clinical trial) for AL002c will be presented at the AAIC 2026 London Annual Meeting via a Late-Breaking Science presentation and a poster session. This marks the first unblinding of Phase II clinical data for a microenvironmental modulation strategy targeting microglia, which will have a decisive impact on the valuation of the entire therapeutic field.
Q: How can blood biomarker testing be used to aid in the early diagnosis of Alzheimer’s disease and patient recruitment for clinical trials?
A: Blood biomarker testing represents one of the most significant advancements in the field of AD diagnosis from 2023 to 2026.Ultra-sensitive detection platforms, such as Quanterix Simoa (single-molecule array technology) and Roche Elecsys pTau217, have increased the detection sensitivity of traditional ELISA by 1,000 to 10,000 times, transforming “detecting AD biomarkers in blood” from a research topic into a clinical reality.
① Significantly reduced patient screening costs: Enrollment screening for traditional AD clinical trials relies on PET scans (approximately $3,000–5,000 per person), whereas blood biomarker testing (pTau-217, Aβ42/40 ratio) costs only $300–600 per person and yields results within one week.Adopting a two-step strategy of “blood-based pre-screening + PET confirmation” can increase clinical trial screening efficiency by 3–5 times and reduce PET usage by over 70%.
② Improve the “true positive rate” of enrolled patients: By using blood pTau-217 or Aβ42/40 ratio for pre-screening, patients with cognitive impairment who “do not have AD pathology at all” (such as those with vascular dementia or Lewy body dementia) can be excluded before they undergo expensive and time-consuming PET scans, ensuring that patients entering the PET confirmation phase have a higher probability of having AD pathology.
③ Enable dynamic pharmacodynamic monitoring: During treatment, regular testing of blood biomarkers such as pTau-217 and NfL (neurofilament light chain) can serve as “real-time feedback signals” indicating whether the drug is slowing neuronal damage.Compared to PET scans, which can only be repeated every 12–18 months, blood tests can shorten the interval for pharmacodynamic follow-up to every 3–6 months, significantly improving the data collection density and efficiency of clinical trials.
④ Driving the Decentralization of AD Diagnosis to Primary Care: Roche’s Elecsys pTau217 received FDA approval in 2024 for theassisted diagnosis of AD. This means that AD diagnosis is no longer limited to a handful of large academic medical centers—community primary care clinics can now collect blood samples, send them to central laboratories for testing, and obtain highly accurate AD risk assessment results.This trend will have a profound impact on the patient recruitment models for clinical trials in AD drug development.
7.0 Disclaimer

This article was written by the editorial team at https://bio-conference.com/ based on publicly available academic materials, conference information, and industry analysis, and is intended solely for academic exchange and industry reference. Any mention of drugs, medical devices, or treatment regimens in this article does not constitute medical advice, investment advice, or commercial recommendations.
The clinical trial data and conclusions described herein are solely a compilation of publicly available information as of Q2 2026. The final results of each clinical trial may be subject to uncertainty; readers should refer to the final review opinions issued by relevant regulatory authorities and the official clinical data published by pharmaceutical companies.
This website, , assumes no liability for any direct or indirect losses arising from the use of the information contained herein.