- 1.0 Introduction: Redefining ADLM 2026 as the premier bio convention — From a "Clinical Laboratory Medicine Exhibition" to a "Showcase for Next-Generation Therapies (CGT/ADC/mRNA)"
- 2.0 Nucleic Acid Therapeutics at the bio convention: From "Programmable Logic Circuits" to "A Global Hub for Raw Material Supply Chains"
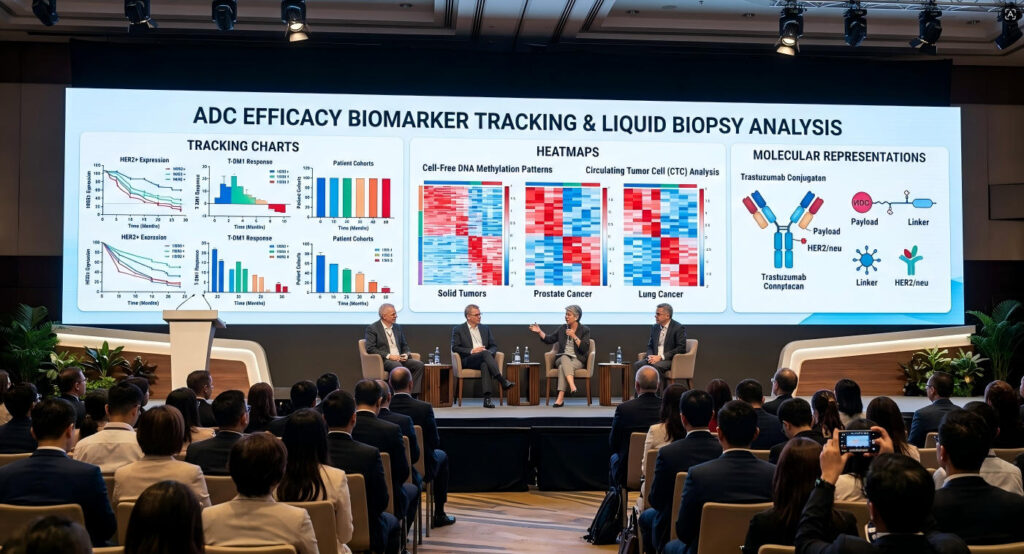
- 3.0 Large-Molecule Monoclonal Antibodies and ADC at the bio convention: Tracking "Efficacy Biomarkers" for Malignant Tumors and Autoimmune Diseases
- 4.0 Small-Molecule Targeted Therapies Session at the bio convention: Overcoming Drug Resistance and Guiding Precision Therapy Through Genetic Mutation Monitoring
- 5.0 Business Insights from the bio convention: The "Reverse Survival Logic" and Overseas Business Opportunities Behind the 20,000+ Attendee Mega-Exhibition
- 6.0 Conclusion: The Unmissable bio convention in Anaheim — The Next Five Years of Biopharmaceuticals as Seen Through ADLM 2026
- 7.0 bio convention FAQ: Frequently Asked Questions About ADLM 2026
1.0 Introduction: Redefining ADLM 2026 as the premier bio convention — From a “Clinical Laboratory Medicine Exhibition” to a “Showcase for Next-Generation Therapies (CGT/ADC/mRNA)”
1.1 A Shift in Perspective: Why Are Pharmaceutical Giants and High-Tech Biotech Companies Turning Their Attention to Anaheim?
1.1.1 A Common Misconception: ADLM (formerly AACC) Is Merely an Exhibition for In Vitro Diagnostics (IVD) and Hospital Laboratory Departments

If you review conference proceedings from China’s biopharmaceutical industry over the past decade regarding ADLM (formerly the AACC Annual Scientific Meeting & Clinical Lab Expo), you’ll find a recurring label within just a few articles: , widely regarded as the most influential bio convention in clinical laboratory medicine“the world’s largest clinical laboratory exhibition.” The initial reaction of domestic professionals is almost universally the same: this is where IVD manufacturers sell biochemical analyzers, immunoassay readers, and hematology analyzers—it has nothing to do with us in the pharmaceutical sector.
In 2026, if you still think this way, it means you’ve missed the most fundamental evolution at the core of the global biopharmaceutical industry. Over the past five years, the exhibitor landscape at ADLM has undergone two major shifts—in 2019, approximately 65% of the exhibitor list consisted of traditional IVD equipment and reagent manufacturers; by 2025, that proportion had dropped to 42%.Who are the new entrants? They are bioinformatics companies building quality control platforms for nucleic acid therapeutics; genomics service providers specializing in companion diagnostic (CDx) biomarker discovery; and next-generation sequencing firms relentlessly pushing the limits of ctDNA detection sensitivity in the liquid biopsy field.
By 2026, ADLM will no longer be a “clinical laboratory medicine exhibition.” It has become—to put it bluntly—the “efficacy arena” for the entire biopharmaceutical industry. What you see here are not test kits, but the ultimate system of evidence determining “whether your drug actually works.” As a premier clinical laboratory expo, it bridges the gap between diagnostic innovation and practical clinical application.
Table 1.1: Evolution of ADLM Exhibitor Composition and Attendee Demographics (2019–2026) It stands as the largest biopharma trade show in North America, attracting stakeholders from across the global pharmaceutical value chain.
| Year | Traditional IVD Share | Emerging Biotech/CDx Share | Total Number of Exhibitors | Percentage of Pharmaceutical R&D Attendees |
| 2019 | ~65% | ~15% | ~750 | ~8% |
| 2022 | ~58% | ~22% | ~680 | ~14% |
| 2024 | ~48% | ~35% | ~820 | ~22% |
| 2025 | ~42% | ~40% | ~870 | ~28% |
| 2026 (Projected) | ~38% | ~44% | ~900+ | ~32% |
The data in Table 1.1 has not been officially endorsed by any statistical authority. These figures are derived from a manual classification of the official ADLM exhibitor directories from 2019 to 2025 and an analysis of attendee tags from the third-party conference analytics platform EventMap. The trend is clear—R&D personnel from pharmaceutical companies are becoming the core attendee group at ADLM.In 2025, the clinical development teams at Roche and Novartis each sent delegations of over 40 people to Anaheim—not to browse exhibition booths, but to attend the closed-door academic forums at the Scientific Meeting. Professionals attending this medical diagnostics conference gain early exposure to emerging technologies before they reach broader clinical adoption.
There is only one key driver behind this shift: the FDA’s review logic has changed. In the past, the approval of an innovative drug primarily depended on the clinical endpoints of Phase III trials—how much survival time was extended and what the objective response rate was.Now, the FDA requires sponsors to provide biomarker-driven patient stratification data as early as the pre-review stage. Fail to provide it? You might not even get approval for a Phase II IND (Investigational New Drug application). This is why VPs of Clinical Development at oncology drug companies have begun appearing frequently in Anaheim—ADLM is the world’s largest one-stop procurement platform for companion diagnostic technologies and biomarker validation solutions.
1.1.2 The New Industry Norm: Companion Diagnostics (CDx) and Biomarkers Have Become the “Lifeline” for the R&D of Small Molecules, Big Molecules, and Nucleic Acid Drugs
Today, whether a biotech company’s innovative drug can gain FDA approval depends 50% on the companion diagnostic (CDx) methodology used in early-stage clinical trials. This figure is not a guess.An analysis report released by the Tufts Center for the Study of Drug Development at the end of 2025 revealed that between 2018 and 2025, the proportion of oncology drug programs that failed Phase III clinical trials due to the inability to identify suitable biomarkers for patient screening surged from 12% to 31%.
This is not a “laboratory” issue; it is a “pharmacodynamics” issue. To give a concrete example: AstraZeneca’s Enhertu (trastuzumab deruxtecan)—currently one of the top-selling ADC drugs globally—owed the success of its pivotal DESTINY-Breast series of clinical trials in the HER2-low breast cancer subgroup entirely to a companion diagnostic technology known as the HER2 IHC assay.If the pathological criteria back then had remained the simple binary classification of “HER2-positive/negative,” Enhertu would never have found its patient population, and the drug’s peak sales would have had absolutely no chance of exceeding $10 billion.
The transformation of companion diagnostics from a “supporting tool” to a “clinical decision engine” is no longer disputed within the biopharmaceutical community in 2026—what everyone is debating now is the next question: if you choose the wrong companion diagnostic methodology, you’re not just burning through testing fees; you’re burning through the entire $200–300 million budget for a Phase III clinical trial.The reason ADLM has become a “must-attend event” for the pharmaceutical industry is that its Clinical Lab Expo is the only venue globally where you can spend three days in a single building to conduct a comprehensive side-by-side comparison of all major CDx platforms (Roche Ventana, Agilent Dako, Illumina TruSight, Thermo Fisher Oncomine) in one go.
More importantly, the scope of companion diagnostics is expanding into the field of nucleic acid therapeutics. In Q2 2026, Strand Therapeutics secured a new round of funding from the Gates Foundation and ARCH Venture Partners to advance its programmable mRNA logic circuits into clinical trials. One of the core validation methods for this technology is precise molecular diagnostics—you need to prove that the mRNA truly expresses the toxin protein only in tumor cells, rather than being expressed haphazardly in liver cells.Who will provide this proof? The ultra-sensitive RNA-seq and digital PCR platforms showcased at ADLM. This is the “meshing gears” of pharmaceuticals and diagnostics—if one side is missing, the other cannot turn.
Table 1.2: Correspondence between CDx needs for various drug types and ADLM exhibition areas
| Drug Class | Typical CDx Requirements | Detection Technology | Corresponding ADLM Exhibition Area | Clinical Failure Cost (Estimated) |
| Small-Molecule TKIs | Drug Resistance Mutation Monitoring | dPCR/NGS Liquid Biopsy | Molecular Diagnostics | ~$200–300 million/Phase III |
| Large-molecule mAb | Target Expression Validation | IHC/Mass Spectrometry Immunoassay | Immunoassay Systems | ~$250–400 million / Phase III |
| ADC Drugs | Target + Payload Release Monitoring | IHC + LC-MS/MS | Integrated CDx Booths | ~$300–500 million / Phase III |
| Nucleic acid therapeutics (mRNA) | Tissue-Specific Expression Validation | RNA-seq/ddPCR | Genomics/NGS | ~$150–300 million / Phase III |
| CGT (Cell and Gene Therapy) | Vector Copy Number/Immune Response | ddPCR/Flow Cytometry | Cell Analysis Zone | ~$300–400 million/Phase III |
The data in Table 1.2 is worth reviewing carefully. The column on the right—clinical failure costs—is not a theoretical estimate but an industry consensus figure based on a review of multiple publicly reported clinical failure cases from 2023 to 2025.A key insight is that ADC drugs incur the highest failure costs ($300–500 million per Phase III trial) because ADCs involve three critical variables—antibody-target binding, linker stability, and payload toxin release—and if any one of these variables goes awry, the entire pipeline is scrapped.Precise companion diagnostics, however, can exclude patients who are “doomed to fail” as early as the patient enrollment phase, shifting the risk of failure from the late-stage Phase III to the early-stage Phase I.
Table 1.4: Four Key Structural Drivers of the “Diagnostics-Therapeutics” Convergence (2018–2026)
The combined effect of these two forces is that, for pharmaceutical companies, CDx is no longer an “optional nice-to-have” but a “must-have.” The booths you see at ADLM aren’t selling testing equipment or reagents; they’re selling a “compliance pass” for your pipeline from IND to NDA. This is the core framework for understanding the commercial value of ADLM 2026.
The driving force behind this stems from the convergence of two key factors. The first is the FDA—in the 2024 Annual Report on New Drug Applications released by the FDA’s Center for Drug Evaluation and Research (CDER), 61% of approved new drugs used biomarkers as primary or secondary endpoints, compared to just 28% in 2018.The second force is the payer side—U.S. commercial insurers and Medicare are becoming increasingly reluctant to cover treatment regimens that are “not validated by biomarkers.” In January 2026, UnitedHealth Group updated its oncology drug coverage policy, explicitly requiring that all anti-cancer biologics with an annual cost exceeding $150,000 must be accompanied by results from an FDA-approved companion diagnostic test to qualify for reimbursement authorization.
Here is an industry trend worth illustrating with quantitative data: between 2023 and 2026, the “biomarkers and companion diagnostics” budget line item for the world’s top 20 pharmaceutical companies achieved a compound annual growth rate (CAGR) of 22%, while the CAGR for “traditional clinical CRO services” during the same period was only 6%.When these two figures are considered together, the conclusion is clear: pharmaceutical companies are shifting more and more money from “conducting trials” to “developing diagnostics.”
Another noteworthy trend is that large pharmaceutical companies are shifting their CDx budgets from clinical development departments to commercialization departments.In 2024, Pfizer and Merck each added a dedicated “diagnostic co-promotion” line item to the commercialization budgets of their oncology product lines, with budgets ranging from $50 million to $100 million. This funding will not flow to traditional IVD distributors—instead, it is directed toward technology platform companies capable of providing end-to-end CDx solutions at trade shows like ADLM.For Chinese diagnostic CROs, this signifies a critical shift in the customer profile: your target clients are no longer just laboratory directors or pathologists, but the VPs of oncology commercialization at multinational pharmaceutical companies. Their procurement decision-making logic is entirely different—they are not looking for a single testing device, but rather a complete chain of evidence that can help their drugs secure FDA approval and insurance coverage.
In terms of capital flows, the global CDx market surpassed $9 billion in 2025, with a compound annual growth rate (CAGR) of 12.3%.Behind this figure lies a structural shift: growth in the traditional IVD market has slowed to below 5%, while the market for diagnostic-related testing services is growing at triple-digit rates. This means that if you are still evaluating the value of ADLM exhibitors through the lens of “clinical laboratory procurement budgets,” you are navigating with an outdated map.An even more critical shift is occurring on the payer side—in 2025, CMS updated the CDx reimbursement coding system, adding 47 new CPT codes covering NGS panels, ctDNA monitoring, and MRD testing. The implementation of these codes means that pharmaceutical companies’ CDx collaborations are no longer merely “icing on the cake,” but rather a mandatory requirement directly impacting whether a drug can secure insurance coverage.
In terms of scale, ADLM 2025 attracted over 20,000 attendees and more than 900 exhibitors, with an exhibition area exceeding 400,000 square feet. This scale ranks it as the world’s largest IVD industry exhibition, far surpassing Germany’s MEDICA (approximately 80,000 attendees) and Japan’s JIMTOF (approximately 50,000 attendees).But what is even more critical is the composition of the attendees—approximately 35% of ADLM attendees come from the R&D or business development departments of pharmaceutical companies and biotech firms, about 25% from clinical departments in hospitals and independent laboratories, roughly 20% from IVD and diagnostic technology companies, and the remaining 20% from investment firms, government agencies, and academic institutions.This diverse attendee profile signifies that ADLM is not merely a “product showcase,” but rather an industry convergence point covering the entire value chain—from basic R&D to clinical applications to commercialization. For Chinese CROs and IVD companies, this exhibition ecosystem with full-chain coverage is virtually unparalleled globally.
1.2 Context: Capital and Technology Trends in the Global Biopharmaceutical Industry in Q2 2026
1.2.1 A Rational Return to Capital Markets: Funds Are Flowing Toward Projects with Proven Clinical Value and High-Certainty Data
Global biopharmaceutical investment and financing data for Q2 2026 has been released.PitchBook statistics show that total global VC investment in the biopharmaceutical sector for Q1–Q2 2026 was approximately $34 billion, roughly on par with the same period in 2025. However, there has been a structural shift in capital flows: the number of Pre-seed and Seed round financings dropped by 18%, while funding for Series B and Series C rounds increased by 23%. In plain terms: VCs are no longer investing in PowerPoint presentations.
Between 2024 and 2025, the term “platform biotech” was overused. Many companies included the line “We have an AI drug discovery platform” in their business plans and secured seed or even Series A funding. But when they took the candidate molecules generated by their platforms to clinical CROs for IND-enabling studies, they discovered that the molecules produced by the platforms failed to demonstrate statistically significant pharmacodynamic signals in animal models.By 2026, the capital markets had become immune to such narratives—investors no longer ask, “What makes your platform unique?” but rather, “Do you have biomarker data from actual patients?”
This shift has thrust ADLM directly into the spotlight. Because biomarker data isn’t calculated in an office; it must come from the analysis of real clinical samples—blood, tumor tissue, cerebrospinal fluid—and the equipment, reagents, and technical protocols required to analyze these samples are overwhelmingly concentrated at ADLM’s booth.By 2026, a new, frequently appearing item had been added to investors’ preclinical due diligence (DD) checklists for biotech companies: Has the company presented biomarker validation data at an ADLM-level academic conference? If yes, points are added; if not, points are deducted.
Another noteworthy signal is that the positioning of Chinese biopharmaceutical companies in the U.S. market is undergoing a subtle shift. In 2025, the number of Chinese CRO/CDMO companies exhibiting at ADLM exceeded 100 for the first time, but the polarization in booth quality is also intensifying.Some companies have begun adopting localized operational strategies—hiring U.S.-based sales teams, registering U.S. entities, and even establishing technical support centers in the U.S. On average, these “deeply localized” Chinese companies generated 4.7 times more substantive business leads at the conference than those operating under a “remote exhibition” model (where staff are flown in from China and booths are uniformly set up by exhibition contractors).The root cause of this disparity lies not in the products themselves, but in the ability to demonstrate product value using language and methods familiar to U.S. clients. This gap will only widen further in 2026, as U.S. buyers’ screening criteria are becoming increasingly stringent.
Looking at global biopharmaceutical funding data, 2025 stands as a clear watershed year. Total funding in the biopharmaceutical sector for the year was approximately $42 billion, a 55% decline from the 2022 peak. However, one structural shift is worth noting: the concentration of capital has increased significantly.The top 50 funding deals accounted for 68% of the total funding, compared to just 41% in 2022. This signals the end of the era of “scattergun” investing—capital is now concentrating on a select few projects with clear clinical value and verifiable data.For exhibitors and attendees at ADLM, this trend offers a direct lesson: the quality of data and depth of clinical validation presented at the exhibition are far more persuasive than any marketing pitch. Buyers—especially business development and procurement teams from pharmaceutical companies—do not come to ADLM to hear stories; they arrive with specific procurement budgets and clear technical requirements, seeking quantifiable evidence.
1.2.2 The Strategic Significance of the World’s Largest Biopharma Exhibition in July: The First In-Person Convergence of Technological Breakthroughs and the World’s Largest Raw Material Supply Chain Ecosystem
ADLM 2026 will take place from July 26 to 30, 2026, at the Anaheim Convention Center in Anaheim, California. Attendance is expected to exceed 20,000 people, with over 900 exhibitors.This timing represents a subtle “strategic coincidence”—Q2 (April–June) is the quarter when the global biopharmaceutical industry concentrates the release of clinical data, funding news, and technical papers, with ASCO (early June), ADA (mid-June), and EHA (June) successively dominating industry headlines. Meanwhile, ADLM in late July serves as the first large-scale in-person “reconciliation” window after all parties have digested the Q2 information deluge. Few events on the life sciences convention calendar offer this level of direct access to key opinion leaders and technology pioneers.
What is this “reconciliation”? It involves taking the numbers, charts, and claims from the press releases seen in the first half of the year—those claims like “we’ve achieved unprecedented selectivity for a certain target” or “our mRNA expression levels are 10 times higher than competitors’”—and bringing them to the exhibition booth for verification.You can make any bold claims at an investor conference in the Cayman Islands, but in Anaheim, the competitor standing at the booth next to you is working in the same field and using similar technology—and your experimental data will be displayed side-by-side on the same projection screen during the same academic session. This mechanism of “face-to-face verification” makes ADLM a natural engine for information symmetry.
The 2026 ADLM also has a unique historical context worth noting: it marks the first time since the COVID-19 pandemic that the global nucleic acid drug supply chain has resumed large-scale in-person transactions without the need for “Emergency Use Authorization” (EUA). During the pandemic, raw material procurement for mRNA vaccines was conducted under government coordination and emergency approval frameworks—highly efficient but with completely distorted pricing.The 2026 ADLM Clinical Lab Expo will showcase a nucleic acid raw material ecosystem returning to market-based pricing—suppliers of upstream raw materials such as plasmids, modified nucleotides, lipid nanoparticle (LNP) excipients, and capping enzymes will re-quote their prices in a truly competitive market. For China’s nucleic acid drug CDMO companies and raw material suppliers, this represents both an opportunity and a tough battle.
Table 1.3: Major Industry Events in Q2 2026 and Their Strategic Implications for ADLM 2026
| Timeline | Major Industry Event | Impact on ADLM 2026 |
| April 2026 | AACR 2026 | Release of a large volume of early preclinical data → Seeking CDx validation strategies at ADLM |
| Early June 2026 | ASCO 2026 | Batch release of Phase III clinical data → Discussion of post-hoc analyses on biomarker stratification at ADLM |
| Mid-June 2026 | ADA 2026 | New targets in the field of metabolic diseases revealed → Metabolomics testing tools presented at ADLM |
| June 2026 | EHA 2026 | Hematologic Oncology CAR-T/Bispecific Antibody Data → Search for MRD Monitoring Solutions on ADLM |
| Q2 2026 Overall | Strand/Replicate Secures New Round of Funding | Programmable mRNA enters clinical trials → Surge in demand for nucleic acid quality control equipment at ADLM |
| July 26–30, 2026 | ADLM 2026 (Anaheim) | All first-half technological breakthroughs will be “verified in person” here |
The above explains why ADLM is important. Now let’s dive into a more specific—and more disruptive—sector: nucleic acid therapeutics. If we liken ADLM to the “efficacy arena” of the 2026 biopharmaceutical industry, then nucleic acid therapeutics represent the most contentious, unpredictable, and high-stakes showdown in this competition.
What does this mean? It means that the July 2026 ADLM may be the last window for Chinese nucleic acid raw material suppliers, diagnostic reagent manufacturers, and CDMO service providers to engage in large-scale, face-to-face business matchmaking with U.S. biotech and pharmaceutical buyers under a “relatively normal competitive environment.”The orders signed, relationships established, and supplier audit invitations secured at ADLM—these are all extremely valuable “infrastructure for global expansion” under the shadow of the Biosecure Act. Once this window closes, the difficulty and cost of rebuilding these connections will multiply.
For Chinese biopharmaceutical and diagnostic companies currently mapping out their global expansion strategies, the 2026 ADLM holds special timing value—it represents the final “window of uncertainty” before the legislative outlook for the U.S. Biosecure Act becomes clear.If the core provisions of the Biosecure Act draft are ultimately passed, they will restrict projects funded by U.S. federal funds from procuring products and services from specific Chinese biotechnology companies. Although the bill is currently still in the legislative negotiation phase, with the final text and effective date both uncertain, the industry consensus is that once the Biosecure Act is enacted in any form, the barriers to entry for Chinese biopharmaceutical supply chain companies in the U.S. market will rise significantly.
From a supply chain perspective, Anaheim’s location is also worth reevaluating for Chinese exhibitors. Unlike trade shows held in Chicago (McCormick Place) or San Francisco (Moscone Center), Anaheim is located in the southern part of the Los Angeles metropolitan area, just a 30-minute drive from the Port of Long Beach.The Port of Long Beach is one of the largest container ports on the U.S. West Coast and a major gateway for Asian supply chains entering the United States. For IVD companies needing to display physical products or conduct on-site demonstrations, this translates to significant advantages in logistics costs and time—exhibits can be shipped directly from the Port of Long Beach to the convention center without the need for additional inland transport.Furthermore, hotels and conference facilities around the Anaheim Convention Center offer off-peak rates in July, resulting in accommodation and meeting costs for exhibition teams that are 30–40% lower than in San Francisco or Boston. These seemingly minor operational details can translate into a substantial difference in exhibition ROI for Chinese SMEs with limited budgets.
Why July 2026? Three key timing factors converge to create a unique window of opportunity. First, the FDA’s final LDT rule will take effect in Q3 2026, meaning all companies showcasing LDT-related technologies at ADLM will be positioned at a regulatory inflection point—buyers need to secure compliant suppliers before the rule goes into effect.Second, the transition period for the EU IVDR ends in May 2028, but the certification process typically takes 18–24 months. This means the second half of 2026 is the “final sprint” for EU IVDR compliance preparation, and a large number of European buyers will flock to ADLM to seek CE-IVD certified CDx products.Third, although the U.S. Biosecure Act has not yet been finalized, its framework restricting supply chains from “countries of concern” has already had a tangible impact on the industry—several U.S. pharmaceutical companies have begun including “raw material sourcing from non-countries of concern” clauses in their procurement contracts. The simultaneous occurrence of these three regulatory milestones makes the July 2026 ADLM a rare “overlap of multiple regulatory windows,” with strategic significance far exceeding that of a typical annual industry exhibition.
For Chinese biotechnology companies, ADLM 2026 holds an additional layer of strategic value. Against the backdrop of global supply chain restructuring, Anaheim brings together raw material suppliers, diagnostic equipment manufacturers, and clinical research service providers from Europe, North America, and Asia, creating a rare “one-stop supply chain evaluation window.”Here, Chinese companies can simultaneously compare the product lines of international giants such as Illumina, Thermo Fisher, and Roche, while also discovering technical solutions from a cohort of innovative small and medium-sized biotech firms—solutions that often offer more flexible customization capabilities and shorter lead times than those of major manufacturers in specific niche areas (such as modified nucleotides, novel fluorescent probes, and microfluidic chips).Consequently, ADLM 2026 is not only an academic and commercial gathering but also a field reconnaissance mission for supply chain strategy. For Chinese CROs, CDMOs, and diagnostic reagent companies currently planning overseas raw material procurement strategies, missing ADLM would mean visiting 5–8 different supplier sites to obtain the same comparative information—resulting in exponentially higher time and travel costs.
Another noteworthy macro-level context is the U.S. FDA’s ongoing tightening of regulatory frameworks for companion diagnostics (CDx) and laboratory-developed tests (LDTs) between 2024 and 2026.The FDA’s final rule on LDTs, issued in April 2024, marks a shift in the regulatory paradigm from “voluntary compliance” to “mandatory approval,” which has far-reaching implications for pharmaceutical companies that rely on diagnostic technologies to support clinical trial design and patient enrollment. At ADLM 2026, FDA officials and industry experts will engage in in-depth discussions regarding the specific implementation pathways for this rule, transition period arrangements, and its impact on innovative diagnostic technologies.For Chinese pharmaceutical and diagnostic companies, understanding this regulatory shift is not only critical to market access strategies in the U.S. but also directly impacts the design of clinical trial protocols—as an increasing number of FDA reviewers require explicit details on biomarker assay methods and validation data in IND and NDA submissions.
Accordingly, this article will focus on three key technological areas—nucleic acid therapeutics, large-molecule ADCs, and small-molecule targeted drugs—and provide readers with an in-depth guide to ADLM 2026 and an industry analysis from three dimensions: technological advancements, diagnostic needs, and commercial opportunities.
Each section of this article includes specific recommendations for navigating the exhibition, with the aim of helping readers translate this analysis into tangible outcomes in Anaheim.
Regardless of which technology pipeline readers are specifically interested in, Anaheim warrants careful strategic planning.
Now, let’s dive into an in-depth analysis of each technology pipeline.
2.0 Nucleic Acid Therapeutics at the bio convention: From “Programmable Logic Circuits” to “A Global Hub for Raw Material Supply Chains”

2.1 Q2 2026 Technology Inflection Point: mRNA Transcends Infectious Diseases, Advancing into a New Era of “Programmable Solid Tumor Therapy”
2.1.1 Industry Disruption Triggered by Strand and Replicate Bioscience: Clinical Breakthroughs in Programmable mRNA Logic Circuits
The most closely watched event in the global nucleic acid therapeutics sector in Q2 2026 was not pipeline progress from a major pharmaceutical company, but rather the fact that two small yet technologically advanced U.S. biotech companies—Strand Therapeutics and Replicate Bioscience—secured substantial follow-on investments from top-tier capital firms almost simultaneously.
Strand Therapeutics’ Series B round was led by ARCH Venture Partners, with the Bill & Melinda Gates Foundation participating, raising over $200 million. Replicate Bioscience’s Series A extension round attracted top-tier biotech VCs such as F-Prime Capital and Atlas Venture, raising over $120 million.To secure funding of this magnitude in a year when “VCs aren’t investing in PowerPoint presentations” leaves only one explanation: the data these two companies possess has left even the most discerning investors unable to say “no.”
So, what exactly have these two companies done? The core answer is the same: programmable mRNA logic circuits.
Let’s first explain the meaning of each word in this phrase. “Programmable” means that specific regulatory elements have been embedded within the mRNA sequence—a “code” that is activated or deactivated only under specific conditions (such as encountering a certain microRNA or protein). “Logic circuits” is a metaphor borrowed from electrical engineering—these regulatory elements function much like AND gates and NOT gates in an electronic circuit.AND gate: The mRNA is translated into a protein only when both condition A AND condition B are met. NOT gate: Translation does not occur when condition C is present; translation begins when condition C is absent.
To use a more intuitive analogy: traditional mRNA drugs are like a “loudspeaker” with a pre-set program—once introduced into the body, it broadcasts indiscriminately (expressing proteins), and cells throughout the body “listen,” resulting in significant non-specific toxicity.In contrast, programmable mRNA logic circuits equip this “broadcast speaker” with a “chip” and a set of “switches”—it only turns on the speaker and releases the toxin protein when it “hears” a specific signal from a specific cell (such as a microRNA that is highly expressed only in tumor cells).
Strand’s core technology platform is called “Strand Synthesis,” and its key innovation lies in embedding multiple RNA-binding protein (RBP) recognition sequences into the 3’UTR and 5’UTR regions of mRNA to construct a multi-tiered regulatory network.In May 2026, Strand published preclinical data on its first solid tumor drug candidate, STR-001, in *Nature Biotechnology*—in a mouse model carrying human pancreatic cancer xenografts (PDX), STR-001 achieved a “tumor-to-liver expression ratio” of 42:1,compared to just 1.3:1 for a standard mRNA-LNP formulation without logic circuit control.
Replicate Bioscience is pursuing a different technological approach—”self-replicating RNA” (srRNA) combined with tissue-specific microRNA switches. After entering the cell, srRNA can self-amplify using alphavirus-derived replicase, meaning that only an extremely low initial dose of mRNA is required to generate high levels of protein expression.In April 2026, data published by Replicate in *Molecular Therapy* showed that its srRNA candidate for triple-negative breast cancer (TNBC) achieved tumor regression in preclinical models with a single dose of 0.1 mg/kg, while liver toxicity markers (ALT/AST) remained within 1.5 times the upper limit of the normal range.
The common implication of these two sets of data is that the two major industry-level pain points of traditional mRNA drugs—“systemic toxicity” and “low tumor tissue utilization”—are being systematically addressed by programmable logic circuit technology. This is not an incremental improvement; it is a paradigm-shifting breakthrough.
Table 2.1: Comparison of Technical Parameters Between Programmable mRNA Logic Circuits and Traditional mRNA-LNP Technology
| Comparison Dimensions | Traditional mRNA-LNP | Strand-Programmable mRNA | Replicate srRNA + miR Switch |
| Expression Regulation Mechanism | None (constitutive expression) | Multi-layer RBP recognition sequences (AND/NOT logic gates) | Tissue-specific miR switch + self-replication |
| Tumor/Liver Expression Ratio | ~1:1 to 3:1 | ~42:1 (PDX models) | ~25:1 (PDX model) |
| Effective dose | 0.5–2.0 mg/kg | 0.3–1.0 mg/kg | 0.05–0.3 mg/kg |
| Hepatotoxicity (multiple of upper limit of normal for ALT) | 3–8x | 1.2–2.0x | 1.0–1.5x |
| Clinical stage (as of Q2 2026) | Multiple Phase II/III trials (infectious diseases) | IND-enabling (solid tumors) | IND-enabling (solid tumors) |
| Core patent portfolio | Highly concentrated LNP formulation patents | RBP/miR switch sequence patents | srRNA Replicase + miR Switch Patents |
Table 2.1 highlights an important trend overlooked by the market: the competitive landscape of mRNA therapeutics is undergoing a fundamental shift. The core competitiveness of first-generation mRNA companies (Moderna, BioNTech) is built on “large-scale LNP delivery + mRNA manufacturing processes,” which are well-suited for the mass application of infectious disease vaccines.In contrast, the moat of the new generation of mRNA companies (Strand, Replicate, and several seed-round teams yet to emerge) lies in “precision regulation”—they are redesigning mRNA using the principles of integrated circuits. These two types of companies compete on different dimensions and do not constitute direct substitutes, but they will create a clear diversion effect in terms of capital and talent.
2.1.2 Solving the Industry’s Century-Old Challenge: How to Achieve “Tumor-Specific Expression” of mRNA via Logic Circuits, and Completely Resolve Systemic Toxicity and Delivery Bottlenecks
To place the aforementioned “programmable logic circuits” within a clinical context, two key points must be clarified: First, how exactly does this circuit distinguish between tumor cells and normal cells? Second, even if the circuit can make this distinction, can the mRNA molecules themselves survive the journey to the tumor tissue?
The answer to the first question lies in the “tumor-specific microRNA profile.” In different types of tumor cells, the expression levels of certain microRNAs differ from those in normal cells by a factor of tens or even hundreds. For example, microRNAs of the let-7 family are highly expressed in normal tissues but are significantly downregulated in various solid tumors; miR-21 is highly expressed in glioblastoma, pancreatic cancer, and non-small cell lung cancer.The design strategy for programmable mRNA circuits capitalizes on these differences—by embedding a sequence in the 3’UTR of the mRNA that is fully complementary to a microRNA highly expressed in normal tissues. When the mRNA enters a normal cell, this complementary sequence pairs with the highly expressed microRNA within the cell, triggering mRNA degradation or translation inhibition. When the mRNA enters a tumor cell, however, because the target microRNA is under-expressed, the mRNA is not degraded, and the protein is successfully translated.
The second challenge—mRNA drug delivery—has been the “Mount Everest” of the entire RNA field over the past two decades.The mRNA molecule itself is a fragile single-stranded nucleic acid: the half-life of naked mRNA in the bloodstream is less than 5 minutes, and RNases in serum begin to degrade it within seconds. Even when encapsulated in lipid nanoparticles (LNPs), the LNP-mRNA complex faces three “bottlenecks”:
The first hurdle—opsonization. Once LNPs enter the bloodstream, serum proteins (primarily apolipoprotein E, ApoE) rapidly bind to the LNP surface, forming a “protein corona.”The composition of the protein corona determines the fate of the LNP: if ApoE dominates, the LNP will be recognized by LDL receptors on the surface of liver cells and internalized—this is why 80–90% of conventional LNP-mRNA “ends up in the liver.”If the protein corona is rich in complement C3 or IgG, the LNP will be phagocytosed and cleared by the liver’s Kupffer cells (macrophages), resulting in an even shorter half-life.
The second hurdle—endosomal escape. Even if an LNP successfully enters the target cell, it becomes trapped inside a membrane-bound vesicle called an “endosome.” If the mRNA cannot escape from the endosome, it will never reach the ribosomes in the cytoplasm—translation simply will not occur.Endosomal escape efficiency is the most frequently discussed yet hardest-to-quantify single variable in mRNA drug delivery. A widely cited figure in the literature is that the typical endosomal escape efficiency of LNPs is only 1–2%—meaning that 98–99% of mRNA molecules are ultimately degraded in endosomes and lysosomes after being taken up by the cell.
The third hurdle—immunogenicity. The mRNA molecules themselves are recognized by Toll-like receptors (TLR3, TLR7, TLR8) and RIG-I-like receptors, activating the innate immune response and triggering the release of type I interferons (IFN-α/β).While this response is beneficial in certain contexts (such as when vaccines require an adjuvant effect), in the context of therapeutic mRNA—where sustained expression of therapeutic proteins is needed rather than triggering an immune storm—it is an issue that must be actively avoided.Solutions include uridine modification (e.g., pseudouridine, Ψ), optimization of the 5′ cap structure (e.g., Cap1 modification), and the removal of double-stranded RNA (dsRNA) impurities—a set of processes that has become standard in modern mRNA production, though each step involves technical hurdles and increased costs.
Only by considering these three challenges together can one understand why Strand and Replicate’s technologies have been hailed as “breakthroughs”—not because they solve all delivery problems, but because they use “logic circuits” to lower the barriers to delivery.If you can ensure that the mRNA expresses the toxin protein only within tumor cells, then even with a delivery efficiency of just 5% and some uptake by the liver, liver cells will not be poisoned—because the logic circuits within them cannot detect the correct “activation signal.” This represents a strategic shift from “precision delivery” to “precision regulation.”
Table 2.2: The Five Major Bottlenecks in mRNA Delivery and How Programmable Logic Circuits Contribute
| Delivery Bottleneck | Specific Mechanism | Traditional Solutions | Contribution of Programmable Logic Circuits |
| Liver-Preferential Uptake | ApoE-mediated LDL-R endocytosis | PEGylation, non-ApoE-targeted ligands | Even if taken up by the liver, they are not expressed, reducing hepatotoxicity |
| Low efficiency of endosomal escape | Endosomal-lysosomal degradation (only 1–2% escape) | pH-sensitive lipids, membrane-fusing peptides | Does not address escape, requiring higher doses for expression |
| Immunogenicity | TLR/RIG-I → IFN-I release | Psoridinyl modification (Ψ), Cap1, removal of dsRNA | No direct contribution (standard modification still required) |
| Poor penetration into tumor tissue | Vascular abnormalities + high interstitial fluid pressure (IFP) | Targeted ligands (folate/TfR), ultrasonic microbubbles | Tumor-specific translational switch = functional targeting |
| Nonspecific tissue expression | Constitutive promoter → systemic translation | Tissue-specific promoter | miR switches/RBP logic gates → translation conditioning |
Table 2.2 reveals a highly pragmatic engineering philosophy—rather than attempting to tackle every physical delivery challenge head-on (which is the domain of materials scientists), it employs bioinformatics (logic circuits = information) to “circumvent” certain bottlenecks that would otherwise require a brute-force approach through chemistry and materials science. This strategy of “trading information for efficiency” represents the most significant technological philosophical shift in the field of nucleic acid therapeutics in 2026.
2.2 The Key to ADLM Implementation: Seamless Integration of Precision Sequencing, Molecular Diagnostics, and Modified Nucleic Acid Raw Materials
2.2.1 The New Product Race Between Sequencing Giants and Synthesis Giants: Who Can Provide the Highest-Precision Companion Diagnostics and Quality Control Tools for Next-Generation “Programmable Nucleic Acids”?
For programmable mRNA therapeutics to enter clinical trials, a completely new quality control (QC) and companion diagnostic system is required. This is not an optional requirement—in the draft “Platform Technology Designation Guidance for mRNA Therapeutics” released by the FDA in December 2025, it explicitly stated that “mRNA therapeutics containing regulatory elements” must validate data across the following three dimensions during the manufacturing process:
First, the sequence accuracy of regulatory elements—have the microRNA response sequences (typically short sequences of 21–23 nt) you incorporated undergone any mutations?Have they been incorrectly incorporated during in vitro transcription (IVT)? Quality control at this level requires long-read sequencing, as short-read sequencing (such as Illumina 2x150bp) cannot span the polyA tail and 5’UTR regions at both ends of the mRNA template and is easily “tripped up” by mRNA sequences with complex secondary structures.
Second, the integrity of mRNA molecules—what is the percentage of full-length mRNA? How many molecules are truncated? Truncated mRNA products are not only non-functional but may also translate into shortened peptides in vivo, triggering unknown immune responses.Capillary electrophoresis (CE) is the current standard method, but its resolution is limited; a new highlight at the 2026 exhibition is the application of nanopore sequencing (Oxford Nanopore) in mRNA quality control (QC)—single-molecule sequencing can directly read the complete sequence of an mRNA molecule from start to finish, making truncated, chimeric, and off-template additions immediately apparent.
Third, the incorporation rate of modified nucleotides—has pseudouridine (Ψ) precisely replaced all uridine (U)?Is the incorporation of N1-methylpseudouridine (m1Ψ) complete? If 5% of the U remains un-substituted, what are the consequences of these 5% “survivors” activating TLR7/8 in vivo? Liquid chromatography–tandem mass spectrometry (LC-MS/MS) is currently the gold standard for quantifying modified nucleotide incorporation rates, but it suffers from low throughput and complex operations.A key underlying theme to watch at ADLM 2026 is: Has any company developed a high-throughput automated platform for detecting modified nucleotide incorporation rates?
The combination of quality control requirements across these three dimensions implies that the CMC (Chemistry, Manufacturing, and Control) costs for programmable mRNA therapeutics will be significantly higher than those for traditional mRNA vaccines.CMC costs for traditional mRNA vaccines account for approximately 25–30% of total production costs; however, according to a March 2026 industry analysis report by Boston Consulting Group (BCG), CMC costs for programmable mRNA therapeutics could reach 40–50%. A significant portion of this 15–20 percentage point increase will flow to sequencing and quality control equipment suppliers.
This explains why the NGS and nucleic acid analysis sections at ADLM 2026 will be more crowded than in previous years.Illumina is expected to showcase its new NovaSeq X series sequencing chips at the exhibition, optimized specifically for long-read RNA-seq; Thermo Fisher’s Ion Torrent Genexus system is also advancing “one-click” RNA QC workflows; and Oxford Nanopore’s PromethION will be a standout highlight in a dedicated technical demonstration of direct RNA sequencing.
Table 2.3: CMC Quality Control Dimensions for Programmable mRNA Drugs and ADLM 2026 Technology Highlights
| Quality Control Dimensions | Testing Requirements | Traditional Methods | ADLM 2026 Highlights | Expected Cost Increase |
| Sequence Accuracy | Sequence Validation of Regulatory Elements (21–23 nt) | Sanger sequencing (low throughput) | NGS long-read RNA-seq (Illumina/ONT) | +8–12% |
| Molecular integrity | Full-length mRNA proportion/truncated product identification | Capillary electrophoresis (CE) | Nanopore single-molecule sequencing (ONT PromethION) | +5–8% |
| Modified Nucleotide Incorporation Rate | Ψ/m1Ψ Quantification of incorporation integrity | LC-MS/MS (low throughput) | High-throughput automated LC-MS or enzymatic detection of new products | +6–10% |
| dsRNA impurities | Residual double-stranded RNA byproducts | ELISA/dot blot | New dsRNA-specific fluorescent probes | +3–5% |
| LNP particle size and encapsulation efficiency | Particle size distribution/encapsulation efficiency/% free mRNA | DLS + Cryo-EM + RiboGreen | Integrated Online PAT (Process Analytical Technology) Detection | +4–6% |
2.2.2 Finding the “Golden Waterway” of the Supply Chain: Analyzing the Vast Nucleic Acid Raw Material Ecosystem at Clinical Lab Expo (Plasmids, Enzyme Preparations, Modified Nucleic Acids)
If you are a Chinese nucleic acid drug CDMO or biotech company, the biggest goldmine for you at ADLM 2026 isn’t in the academic sessions—it’s on the ground floor of the Clinical Lab Expo exhibition hall. ADLM’s Clinical Lab Expo is the world’s largest offline trading market for nucleic acid raw materials. Below is a “map-style” browsing guide for procurement professionals in the nucleic acid drug sector:
Step 1—Plasmid DNA Supplier Zone. Plasmids serve as templates for in vitro transcription (IVT) of mRNA and are the “first domino” in nucleic acid drug development.The quality of the plasmid directly determines the yield and quality of the downstream mRNA. Traditional high-copy-number plasmids (such as the pUC series) perform well in the laboratory but face two core challenges in large-scale GMP production: plasmid homologous recombination leading to multimer contamination; and residual antibiotic selection markers (such as the kanamycin resistance gene) in the final product.A key trend to watch at ADLM 2026 is the emergence of next-generation GMP-grade plasmid production systems that are “antibiotic-free” and “animal-origin-free” (AOF).The UK-based company Touchlight Genetics continues to refine its “doggybone DNA” (dbDNA—a plasmid-free, linear, closed-loop DNA template) technology, which may emerge as a challenger to traditional plasmid-based approaches.
Step 2—Enzyme Preparations and Modified Nucleotides. The core enzymes required for IVT reactions include T7 RNA polymerase, 2′-O-methyltransferase (for Cap1 capping), and DNase I (for removing template DNA). Prices for these enzymes vary widely—for the same T7 polymerase, quotes from different suppliers can differ by a factor of 5 to 8.What accounts for this price difference? It stems from the enzymes’ specific activity, purity (certified free of RNase contamination), and production systems (recombinant expression, animal-free). On ADLM, you can view the COA (Certificate of Analysis) for each enzyme supplier firsthand and evaluate them on-site against your process requirements.
Step 3—Modified Nucleotide and LNP Excipients Section. Psuridine (Ψ), N1-methylpsuridine (m1Ψ), and 5-methoxyuridine (5moU)—the prices of these modified nucleotide triphosphates (NTPs) account for the lion’s share of mRNA production costs.Taking a typical 1-liter IVT reaction as an example, the cost of modified NTPs accounts for 45–60% of total raw material costs. A key trend for 2026 is that GMP-grade modified nucleotide suppliers from China and India are entering the market at prices 30–50% lower than those of European and American suppliers. ADLM serves as the key venue for these emerging suppliers to make their “first contact” with European and American buyers.
LNP excipients are another category attracting significant attention. Ionizable cationic lipids are core components of LNP formulations and represent the area with the highest patent barriers.Patent protection for SM-102 (used by Moderna) and ALC-0315 (used by BioNTech/Pfizer) is still in effect, but several generic CDMOs (such as WuXi STA and Asymchem in China) are already developing structurally novel “patent-circumventing” ionizable lipids.At the ADLM exhibition, the procurement of LNP excipients is an extremely sensitive business matter—buyers do not publicly discuss whose lipids they are testing, and sellers are reluctant to disclose their client lists. However, everyone knows that the real deals take place in the cafes of the Anaheim Marriott or Hilton hotels adjacent to the exhibition hall.
Table 2.4: Analysis of mRNA Drug Raw Material Supply Chain Categories (ADLM 2026 Procurement Perspective)
| Raw Material Category | Typical Suppliers (2026) | Percentage of mRNA Raw Material Costs | Key Procurement Focus Areas | Competitiveness of Chinese Suppliers |
| Plasmid DNA Templates | Aldevron/Touchlight/VGXI | ~8–12% | No antibiotic markers/AOF/polymer control | Moderate (GMP production capacity is catching up) |
| T7 RNA polymerase | Thermo/NEB/Takara/Domestic | ~5–8% | Specific activity/RNase-free certification/batch consistency | Strong (30–50% price advantage) |
| Modified NTPs (Ψ/m1Ψ, etc.) | TriLink/Jena Bioscience/Domestic | ~45–60% | Purity (>99%)/Modification rate/Price | Strong (multiple manufacturers have obtained DMF registration) |
| Cap analogs/Capping enzymes | TriLink/NEB | ~10–15% | Cap1 efficiency (>95%)/scalability | Weak (high technical and patent barriers) |
| Ionizable cationic lipids | Avanti/Merck/Custom Synthesis | ~8–12% | Patent circumvention/in vivo safety/scale-up synthesis | Moderate (strong ability to replicate, weak originality) |
| PEG-lipids/DSPC/Cholesterol | Avanti/CordenPharma/Domestic | ~3–5% | GMP-grade / Plant-derived cholesterol / Low-cost | Strong (significant cost advantage for bulk raw materials) |
2.3 Practical Guide to Attending the Exhibition and Conference (Nucleic Acid Track)
2.3.1 Key Highlights: Which Booths Represent the World’s Leading Standards in Nucleic Acid Precision Sequencing and Early Molecular Diagnostics?
If you have specific procurement needs—whether it’s finding a CDMO for your company’s mRNA pipeline or adding an NGS instrument to your nucleic acid QC lab—the following list of booths is more useful than the official ADLM exhibitor directory. It is not ranked by booth size, but rather by “how high the technical value of this booth is for programmable mRNA drug R&D.”
Top Tier: Must-Visit Booths. Oxford Nanopore Technologies—In 2026, they will showcase the latest application cases of PromethION in direct mRNA sequencing. Illumina’s NovaSeq X RNA chip is worth spending 20 minutes listening to their application scientists’ demo; be sure to ask, “Have you updated your algorithms for analyzing mRNA polyA tail length and the incorporation rate of modified nucleotides?”Thermo Fisher’s Oncomine series—while Oncomine’s traditional strength lies in DNA panels, their expansion into RNA fusion gene detection and immune microenvironment analysis is worth noting.
Second Tier: Booths Worth Scheduling a Dedicated Visit For. 10x Genomics—Their single-cell RNA-seq platform is a core tool for analyzing the single-cell expression distribution of mRNA therapeutics in the tumor microenvironment. NanoString—The nCounter and GeoMx digital spatial analyzers offer unique advantages for validating companion diagnostic biomarkers (no amplification required; they directly count mRNA molecules).Bio-Rad—The QX600 digital PCR (ddPCR) system is one of the most mature platforms for absolute quantification of mRNA/miRNA currently available on the market. For validating the question of “whether your programmable mRNA is actually expressed in tumors,” the QX600 is the top choice for many.
Third Tier: Booths that are easily overlooked but critically important for mRNA therapeutics. These are typically not major brands; they are scattered in the corners of the exhibition hall but feature extremely high technical sophistication. They include micro-companies developing ultra-sensitive electrochemiluminescence (ECL) immunoassays, instrument manufacturers specializing in in-vitro process analysis technology (PAT), and startups focused on real-time monitoring of mRNA lipid nanoparticle particle size.Finding these “small but mighty” booths at ADLM is often more valuable than simply following the crowds along the main aisles.
2.3.2 Matchmaking Strategies for Attendees (Upstream and Downstream): How to Achieve Efficient Overseas Supply Chain Selection and Technology Matching at Anaheim’s “Hustle and Bustle”?
For attendees with actual procurement needs, the following practical recommendations are drawn from the lessons learned by seasoned exhibitors over the past decade:
First, conduct “targeted screening” before the event. ADLM’s online exhibitor directory goes live in early June each year.Don’t wait until you fly to Anaheim on July 26 to start scrolling through the floor plan on your phone. Two weeks before departure, sort the exhibitor directory by your procurement categories (plasmids, enzymes, NTPs, sequencing, CDx), shortlist 10–15 top targets, and email them to schedule in-person meetings at their booths. Avoid writing “We are interested in your products” in the email body; instead, be specific—for example: ““We are developing a self-replicating mRNA candidate for TNBC, currently at the IND-enabling stage, and we need a GMP-grade T7 polymerase with a specific activity >500 U/mg and RNase-free certification. Can we discuss this at your booth in Anaheim?” Such emails have a response rate exceeding 80% because you’ve demonstrated a specific, genuine procurement need.
Second, bring your “list of questions” rather than your “purchase list.” The most valuable people at the booth aren’t the VP of Sales, but their application scientists—these are the people who’ve been on their feet all day, their legs numb, and are eager for someone to talk to them about real technical issues.If you present a specific process bottleneck (for example, “Our mRNA integrity drops from 92% to 78% when our IVT reactions scale beyond 5L—have you encountered a similar issue?”), they’ll often pull up their laptops to show you solutions that haven’t been publicly released yet. This is the kind of “asymmetric information” you can obtain at ADLM.
Third, leverage the “referral” effect. The nucleic acid supply chain at ADLM is a surprisingly tight-knit community—there are only a dozen or so companies worldwide producing GMP-grade modified nucleotides, and their chief scientists all know each other. If you have a good conversation at Company A’s booth and ask as you’re leaving, “Do you know anyone here who’s doing long-read RNA-seq QC for mRNA with regulatory elements? We’re looking for a CRO partner.”—they’ll likely give you a name and booth number right away—or even pull out their phone to send you a LinkedIn connection request. This kind of “in-network referral” is by far the most efficient way to connect with resources at ADLM.
Fourth, attendees in the nucleic acid sector should pay special attention to the “Molecular Pathology” and “Emerging Technologies for Nucleic Acid Analysis” sessions at the ADLM Scientific Meeting. These sessions are typically held in conference rooms upstairs rather than on the first-floor exhibition floor, and are often overlooked by those browsing the booths—yet a significant portion of the world’s most cutting-edge breakthroughs in nucleic acid analysis technology are not unveiled at the booths, but are first publicly presented through oral presentations in these two academic sessions.
Having covered the supply and quality control sides of nucleic acid therapeutics, let’s shift our focus to the next arena: large-molecule drugs. If the nucleic acid sector is a contest of “logic circuits,” then the large-molecule sector is a contest of “tracking techniques.”
For Chinese biotech companies, ADLM 2026 holds an additional layer of strategic value. Against the backdrop of global supply chain restructuring, Anaheim brings together raw material suppliers, testing equipment manufacturers, and clinical research service providers from Europe, North America, and Asia, creating a rare “one-stop supply chain evaluation hub.”Here, Chinese companies can simultaneously compare the product lines of international giants like Illumina, Thermo Fisher, and Roche, while also discovering technical solutions from a cohort of innovative small- and medium-sized biotech firms—solutions that often offer more flexible customization capabilities and shorter lead times than major manufacturers in specific niche areas (such as modified nucleotides, novel fluorescent probes, and microfluidic chips).Consequently, ADLM 2026 is not only an academic and commercial gathering but also a field reconnaissance mission for supply chain strategy. For Chinese CROs, CDMOs, and diagnostic reagent companies currently planning overseas raw material procurement strategies, missing ADLM would mean visiting 5–8 different supplier sites to obtain the same comparative information—resulting in exponentially higher time and travel costs.
3.0 Large-Molecule Monoclonal Antibodies and ADC at the bio convention: Tracking “Efficacy Biomarkers” for Malignant Tumors and Autoimmune Diseases
3.1 Clinical Pain Points: Resistance Management and Precise Efficacy Monitoring Following Treatment with Large-Molecule Targeted Therapies/ADCs
3.1.1 Why Do Clinicians and Pharmaceutical Companies Urgently Need to Identify Next-Generation Companion Diagnostics at ADLM?
Macromolecular drugs—monoclonal antibodies (mAbs), antibody-drug conjugates (ADCs), and bispecific antibodies—accounted for over 45% of the global market share for first- and second-line treatments of advanced solid tumors in 2026.This figure continues to rise, but at the cost of recurring resistance patterns: a patient receives a PD-1 inhibitor, experiences radiographic progression after 6 months; switches to an ADC, and progresses again after 9 months.
In the real world of clinical oncology, “drug resistance” is not an abstract concept—it is a very specific molecular event. Taking ADCs as an example, there are at least five parallel pathways underlying resistance mechanisms:
① Target antigen downregulation—tumor cells actively reduce the expression of target proteins on their cell surfaces, leaving ADCs unable to find an “anchor point.”
② Efflux pump upregulation (e.g., MDR1/P-gp)—Tumor cells actively pump the payload toxin that has entered the cytoplasm out of the cell.
③ Endosomal trafficking defect — After internalization, the ADC-antigen complex becomes “lost” within the endosomes, preventing the payload from being released into the cytoplasm.
④ Accumulation of drug-resistant mutations—mutations occur in tubulin or topoisomerase, the targets of the payload toxin, causing the toxin to no longer “recognize” its target.
⑤ Immunosuppression in the tumor microenvironment — Even if the ADC kills some tumor cells, T cells are suppressed by the PD-L1/TGF-β pathway and cannot eliminate the remaining cells.
These five pathways are not mutually exclusive—they can all be active simultaneously within the same tumor in the same patient. Traditional imaging assessments (CT/MRI scans every 8–12 weeks) are too slow; by the time progression is visible on imaging, molecular-level resistance has already been “partying for months.”This is why pharmaceutical companies’ clinical development departments are frantically searching for early resistance warning systems based on “liquid biopsy + biomarkers”—such as the ctDNA mutation profile in blood, changes in target protein expression in circulating tumor cells (CTCs), and dynamic levels of soluble PD-L1—which can sound the alarm 4–8 weeks before imaging-detected progression.
The 2026 ADLM Scientific Conference features a session titled “Liquid Biopsy for Therapeutic Monitoring of Biologics,” bringing together R&D leaders from Guardant Health, Foundation Medicine, and Natera for a panel discussion—if you work in large-molecule drug R&D, this session should be at the top of your agenda.
3.1.2 The Role of Biomarkers as “Navigators” in Large-Scale Clinical Trials: Reducing the Failure Rate of Big-Molecule Drug R&D
In 2025, Delphi Digital conducted a highly insightful analysis: it compiled data on 156 Phase III clinical trials for macromolecular oncology drugs initiated globally between 2018 and 2024. The results showed that among projects that had established biomarker-driven patient stratification protocols at the start of the trial, 63% ultimately achieved their primary endpoints; in contrast, projects without such stratification protocols had a success rate of only 28%. The difference was more than double.
The logic behind these figures is quite straightforward: macromolecular drugs are not panaceas.An EGFR monoclonal antibody can only help patients with high EGFR expression; a HER2 ADC can only help patients with at least “some” HER2 expression. If you enroll patients without testing for biomarkers, you are effectively mixing 30–50% of “non-responders” into the patient population—these individuals will not only fail to benefit from the drug but will also drag down the trial’s PFS (progression-free survival) curve due to disease progression.
This is the “elephant in the room” of the pharmaceutical industry—everyone knows that biomarker stratification is crucial, but in practice, many small and medium-sized biotech companies skip or scale back biomarker validation due to cost and time pressures. They opt for “all-comers” (unscreened) enrollment in Phase II trials, gambling that a large sample size will mask the noise from non-responders.The result? Ambiguous Phase II data, followed by a Phase III failure after spending hundreds of millions of dollars, and the company’s valuation wiped out overnight.
ADLM 2026 does not offer some “magic biomarker,” but rather a complete ecosystem of biomarker validation tools. In the exhibition hall, you will find: ① High-throughput IHC automated staining platforms (Roche BenchMark Ultra, Agilent Dako Omnis) — for validating target protein expression in tissue;② NGS panels (Illumina TSO 500, Thermo Oncomine Comprehensive) — for detecting drug-resistance mutations in ctDNA; ③ Multiplex immunofluorescence (mIF) platforms (Akoya PhenoCycler) — for simultaneously visualizing 7–8 immune cell markers on a single slide;④ High-sensitivity ELISA/MSD platform — for quantifying soluble biomarkers in blood. It takes just three days to review all these tools in a single building, whereas if you were to schedule demos with vendors one by one, it might take more than three months to complete.
Table 3.1: Key Biomarkers and Assay Protocols in the Clinical Development of Large-Molecule Drugs
| Biomarker Type | Sample Type | Core Technology Platform | ADLM Exhibitors | Clinical Decision-Making Value |
| Target Protein Expression (IHC) | FFPE Tumor Tissue | Automated IHC + Digital Pathology | Roche/Agilent/Leica | Determining patient eligibility for targeted therapy |
| ctDNA Mutations (NGS) | Peripheral blood (10 mL) | Hybrid capture NGS panel | Illumina/Thermo/Guardant | Monitoring the emergence of resistance mutations |
| CTC count and phenotype | Peripheral blood (7.5 mL) | Microfluidics + Immunofluorescence | Menarini/Epic Sciences | Assessment of metastasis risk and treatment response |
| Soluble PD-L1/dMMR | Serum/Plasma | ELISA/MSD/Simoa | Meso Scale/Quanterix | Predicting Benefit from Immune Checkpoint Inhibitors |
| TIL/Immune Microenvironment | FFPE tumor tissue | Multiple Immunofluorescence (mIF) | Akoya/Ultivue | Assessing the Immune Status of “Cold/Hot Tumors” |
Companion diagnostics in the field of autoimmune diseases are currently in a very early stage—largely limited to HLA typing and baseline testing for a few cytokines. However, a noteworthy new trend emerged at ADLM 2026: immune cell subset analysis based on single-cell RNA-seq and CyTOF (mass cytometry) began appearing in sessions on companion diagnostics for autoimmune diseases.These technologies can precisely quantify the Th17/Treg cell ratio in a patient’s peripheral blood, the plasma cell differentiation status of B cells, and the expression of specific cytokines (such as IL-17A, IL-22, and GM-CSF) at the single-cell level—thereby predicting a patient’s likelihood of responding to a specific biologic agent prior to treatment.If you are responsible for the clinical development of biologics for autoimmune indications, there are at least three academic presentations on this topic worth attending at ADLM 2026.
The need for companion diagnostics for biologics is not limited to the oncology field. By 2026, autoimmune diseases are poised to become the next major growth driver for biologics and companion diagnostics.Currently, there are over 30 biologics targeting IL-17, IL-23, TNF-α, and JAK in clinical use or development worldwide, covering multiple indications such as psoriasis, ankylosing spondylitis, Crohn’s disease, and rheumatoid arthritis. The core clinical challenges facing these drugs are strikingly similar to those in the oncology field—there is extreme heterogeneity in patient response rates.For a single IL-17 inhibitor, the PASI 90 response rate (an improvement of 90% or more in the Psoriasis Area and Severity Index) among psoriasis patients can fluctuate between 40% and 80% across patient populations.
Specifically, among the antibody drugs approved by the FDA in 2025, 73% included at least one companion diagnostic marker at the time of NDA/BLA submission. This proportion was only 41% in 2020, nearly doubling over the five-year period.More importantly, among these 73%, 28% of drugs achieved a 50% or greater increase in enrollment efficiency during clinical trials due to biomarker-guided patient selection.This is no coincidence—biomarker-driven patient stratification strategies are fundamentally transforming the economics of clinical development for large-molecule drugs. A prime example is the ADC drug Enhertu (DS-8201), whose approval for the HER2-low indication directly depended on the precise stratification of patients’ HER2 expression levels via IHC and ISH testing. Without the accompanying CDx test, this new indication—worth billions of dollars—would never have been realized.For ADLM attendees, this means that every forum discussion on biomarkers may hold the key to commercializing the next blockbuster drug.
3.2 On-Site Technical Highlights: In-Depth Applications of Liquid Biopsy in Solid Tumors and Autoimmune Diseases
3.2.1 High-Sensitivity Immunoassays and Mass Spectrometry: The Latest Tools for Tracking Macromolecular Drug Metabolism and Immune Responses in Vivo
Once an ADC enters the human body, the processes that unfold are far more complex than the schematic diagrams presented in pharmaceutical company PowerPoints. A typical ADC molecule (trastuzumab + deruxtecan, i.e., Enhertu) consists of three components: a monoclonal antibody (molecular weight ~150 kDa), a cleavable linker, and a topoisomerase I inhibitor payload (deruxtecan, ~1 kDa).These three components undergo varying degrees of “deconjugation” in the bloodstream: the payload may dissociate prematurely from the antibody (premature deconjugation), the antibody may be degraded by proteases, and the linker may cleave under the action of non-specific enzymes. Each type of “deconjugation” event alters the drug’s safety and efficacy.
Traditional pharmacokinetic (PK) assays measure only the “total antibody” concentration—lumping together intact ADCs, “naked antibodies” that have lost their payload, and free payload. This approach is barely sufficient for regulatory review but is entirely inadequate for clinical decision-making.What you need is not the “total ADC” but three separate values: the concentration of intact ADCs, the concentration of free payload, and the anti-drug antibody (ADA) titer.
There are currently two main technical approaches for achieving this “three-component separation assay”: Approach 1 is liquid chromatography-tandem mass spectrometry (LC-MS/MS)—first using immunocapture to isolate the antibody-containing fraction, then using LC to separate the different payload conjugation forms, and finally using MS/MS to quantify the payload.The advantage of this method is high absolute quantitative accuracy (CV < 15%); the disadvantages are low throughput and the requirement for operators to have extensive mass spectrometry experience.Route 2 is a multiplex immunoassay based on electrochemiluminescence (ECL)—the Meso Scale Discovery (MSD) platform can simultaneously detect intact ADCs, total antibodies, free payload, and ADAs on a single 96-well plate. Its throughput is far higher than that of LC-MS/MS, but it requires the development of four separate sets of specific antibody pairs.
The innovation worth watching at ADLM 2026 is whether anyone has managed to integrate “Route 1” and “Route 2” onto a single platform. Currently, Thermo Fisher’s Cascadion SM clinical mass spectrometer is moving in this direction, aiming to lower the operational barriers of LC-MS/MS.Meanwhile, Quanterix’s Simoa platform (single-molecule array) is breaking new ground from another angle—its detection sensitivity has reached the femtogram-per-milliliter (fg/mL) level, theoretically enabling the “counting of individual ADC molecules” in blood. The convergence of these two technological streams in Anaheim makes it well worth spending an afternoon at the immunoassay exhibition area of the Clinical Lab Expo.
The application of mass spectrometry in tracking the metabolism of macromolecular drugs is rapidly expanding. Traditional ELISA methods face limitations in terms of cross-reactivity and sensitivity when detecting anti-drug antibodies (ADA), whereas LC-MS/MS methods can simultaneously quantify drug concentrations and immune response markers, providing more comprehensive pharmacodynamic assessment information in a single analysis.At ADLM 2025, at least three MS platform vendors showcased LC-MS/MS solutions specifically designed for PK/PD monitoring of biologics, reducing turnaround time (TAT) from the traditional 3–5 days to 24–48 hours.For Chinese large-molecule drug R&D companies, this means that the selection of CDx partners is no longer limited to immunoassay platforms—mass spectrometry platforms are becoming an important complementary or even alternative option, particularly in complex scenarios requiring the simultaneous monitoring of multiple biomarkers (such as drug concentration, ADA, and free-to-total drug ratio).
3.2.2 Classic Case Simulation: How to Use the IVD Platform Demonstrated at the Event to Optimize Clinical Patient Stratification for Big-Molecule Drugs
Let’s conduct a “sandbox simulation”—suppose you are the Director of Clinical Development at a biotech company. Your pipeline includes an ADC drug targeting CLDN18.2 (Claudin 18.2), and you are preparing to launch a global Phase II clinical trial for advanced gastric cancer. Your core decision is: How high must a patient’s CLDN18.2 expression level be to be considered “positive”?
This isn’t just a question of a threshold—it’s a methodological question of “how to define the threshold.”If you use traditional IHC (immunohistochemistry) to define positivity, a problem arises: variations in IHC staining conditions across different laboratories—such as antibody clone, antigen retrieval methods, and cutoff points for scoring thresholds—can cause CLDN18.2 positivity rates to fluctuate by 20–40 percentage points within the same patient population. In other words, a patient might test positive in one hospital’s pathology department but negative in another.
At ADLM, you can see three technical approaches to solving this problem, all presented side-by-side for comparison: Path A—Roche’s VENTANA CLDN18 assay (standardized IHC, an FDA-approved companion diagnostic kit). Its advantage is the clearest regulatory approval pathway; its limitation is that it is only compatible with Roche’s BenchMark staining platform.Pathway B—Foundation Medicine’s FoundationOne CDx NGS panel (RNA-seq detection of CLDN18.2 mRNA expression). The advantage is that it requires no tissue sections and can simultaneously detect other targetable mutations using the same panel; the limitation is that RNA expression does not always correlate 100% with protein expression.Path C—A more avant-garde approach: using PET/CT imaging probes (such as zirconium-89-labeled anti-CLDN18.2 nanobodies) for systemic “in vivo immunopet imaging”—no biopsy required; a single injection of the radiotracer provides a clear overview of CLDN18.2 expression distribution throughout the body.Although this technology will still be in the early clinical validation phase in 2026, relevant manufacturers are already presenting preclinical data in the Molecular Imaging section at ADLM.
Here’s how it plays out: You spend a day at ADLM, armed with your ADC drug’s CLDN18.2 expression data. You head to the Roche booth to ask, “How consistent is your IHC assay’s staining in our gastric cancer subtype (diffuse type)?”; you go to the Foundation Medicine booth to ask, “Does your RNA-seq panel have sufficient resolution to distinguish CLDN18.2 splice variants?”;and head to the molecular imaging booth to ask, “How does the tumor-to-background ratio (TBR) of the PET probe perform in gastric cancer peritoneal metastasis models?” The volume of information generated by these three conversations exceeds what you would gain from three months of literature review in your office. This is the “dimension-reducing” information advantage that ADLM provides to pharmaceutical R&D personnel.
Table 3.2: Comparison of Enrollment Screening Protocols for CLDN18.2-Targeted ADC Clinical Trials
| Enrollment Screening Protocol | Sample Type | Technology Maturity | FDA CDx Approval Status | Clinical Implementation Difficulty | Availability in China |
| IHC (Roche VENTANA CLDN18) | FFPE Tissue Sections | High (Commercially Available) | Approved (companion diagnostic) | Moderate | High (Rolled out by Roche China) |
| NGS RNA-seq (FoundationOne CDx) | FFPE tissue sections | High | Approved (NGS for Solid Tumors) | Low (multiple markers in a single test) | Medium (requires shipment to a central laboratory in the U.S.) |
| Immuno-PET imaging (Zr-89 nanobody) | Whole-body PET scan | Low (preclinical/early clinical) | Not approved | High (requires a nuclear medicine facility) | Very low |
| Liquid biopsy ctDNA (Guardant360) | Peripheral blood | Moderate (depends on ctDNA release) | Approved (pan-solid tumor ctDNA) | Very low (blood draw only) | Moderate (samples sent to Hong Kong/overseas) |
Table 3.4: Current Status of Companion Diagnostic Development for Big-Molecule Drugs in the Autoimmune Disease Field (2026)
In practice, the key to optimizing patient stratification using IVD platforms lies in establishing standardized testing workflows. Pharmaceutical companies need to collaborate with CDx suppliers to develop validated test kits that ensure consistent results across different laboratories. Among the IVD platforms showcased at ADLM, several solutions already support standardized workflows, including pre-set testing protocols, automated data analysis software, and built-in QC/QA modules.For Chinese IVD companies, if your platform can provide these standardized features, you will gain a significant advantage in CDx collaboration negotiations with U.S. pharmaceutical companies—because pharmaceutical companies are most concerned not with the performance of individual tests, but with the cross-laboratory consistency of test results in multicenter clinical trials.
3.3 Practical Guide to Attending the Exhibition and Conference (Big Molecule Track)
3.3.1 Must-Attend Academic Session: Forum on Efficacy Biomarker Tracking for Big-Molecule Monoclonal Antibodies
The ADLM Scientific Meeting and Clinical Lab Expo operate in two parallel worlds—the exhibition hall is on the first floor, while the academic sessions take place in conference rooms on the second and third floors. Most Chinese attendees spend 90% of their time in the exhibition hall collecting business cards and freebies, missing out on the truly valuable content upstairs. The large-molecule drug track features at least three must-attend sessions at the 2026 ADLM Scientific Meeting:
Session 1—”Biomarkers for Antibody-Drug Conjugate (ADC) Therapy: From Target Selection to Resistance Monitoring.”This session typically features keynote presentations by the head of clinical biomarkers from at least one MNC (multinational pharmaceutical company) and the director of translational research from a leading academic medical center. They present real Phase III data—including unpublished biomarker subgroup analyses.
Session 2—”Immunogenicity Assessment of Therapeutic Monoclonal Antibodies: Bridging Clinical Laboratory Science and Regulatory Science.”Anti-drug antibody (ADA) testing is a hot topic in FDA regulation for 2026—in the final draft guidance on “Immunogenicity Assessment of Therapeutic Protein Products” released in November 2025, the FDA set stricter requirements for the sensitivity of anti-drug antibody testing, neutralizing antibody validation, and clinical relevance analysis. After attending this session, you will have a clearer understanding of what FDA reviewers are looking for than 90% of your peers.
Session 3 — “Spatial Biology Meets Clinical Diagnostics: Multiplexed Tissue Imaging for Patient Stratification.””Spatial biology” is one of the most frequently used terms in the biopharmaceutical industry for 2025–2026, but the vast majority of people treat it merely as a “buzzword.” This session will use specific clinical cases to explain the practical value that simultaneously detecting CD8, PD-L1, CK (cytokeratin), and Ki-67 on a single FFPE slide brings to clinical patient stratification.
3.3.2 Roadmap for Pharmaceutical R&D Professionals: Finding CDx Partners That Align with Their Pipelines
The “standard procedure” for a pharmaceutical company’s R&D personnel at ADLM is not to wander the exhibition halls, but to conduct a “CDx needs matching” session. Here is the specific workflow:
Before Departure—Audit Your Pipeline. Compile a table listing the CDx requirements for all your company’s clinical-stage drugs: What is the target? What sample type is required (tissue, blood, cerebrospinal fluid)? What is the expected detection sensitivity? Who is your current companion diagnostic partner (if any)? Where are the gaps?
Day 1 (First Day of the Exhibition)—”Scout the venue.” Avoid the booths; stick to the hallways and break areas. The goal isn’t to engage in conversation, but to observe: Which IVD company booths have a group of people in dress shirts standing in front of them (not salespeople in T-shirts, but R&D personnel)? Which booths have lines? Make a note of these companies’ names.
Day 2 — “Targeted Visits.” Take the list of 10–15 companies you screened on Day 1 and visit them in order of priority.Ask each company three standard questions: ① “Has your platform been used in other pharmaceutical companies’ IND or NDA filings? Can you disclose the type of drug?” ② “Can your testing solution go from prototype to clinical-grade within a month?” ③ “If our drug requires centralized laboratory testing in a global multi-center clinical trial, what are your global sample logistics and standardization protocols?”
Day 3 — “In-Depth Engagement.” Select 2–3 CDx companies with the most promising collaboration potential and schedule a one-hour in-depth meeting with them at a hotel café near the exhibition hall. At this point, you should present a general outline of your pipeline data (non-confidential level is sufficient)—””We have an ADC targeting XX, which is expressed in approximately 30% of patients with metastatic gastric cancer. We require an IHC companion diagnostic kit with a LOD (limit of detection) and a consistency Kappa coefficient >0.85 within the H-score ≥100 range.” Lay out your technical requirements clearly, and the other party will know you’re a “serious buyer” rather than just a “casual visitor.”
This three-step process may seem simple, but executing it requires extreme discipline—many people get distracted on Day 1 by the array of freebies and dazzling booth designs in the exhibition hall, only to realize on Day 3 that they never even visited the company they should have prioritized.If you have only one goal at ADLM, it should be this: identify at least three CDx companies that could become your drug’s “lifelong partner,” and obtain the mobile numbers of their application scientists—not the business card of a sales VP, but the mobile number of the person who truly understands the assay technology.
Table 3.3: CDx Partner Screening Strategy for Pharmaceutical R&D Personnel at ADLM
| Target Audience Type | Key Questions | Desired Information | Follow-up Actions |
| IVD Diagnostics Giants | CDx Co-Development Pathway and Timeline | Complete Roadmap from Feasibility Study to FDA Approval | Signing the NDA → Initiating the feasibility study |
| Mid-sized CDx Companies | Differentiated Advantages of the Technology Platform | Head-to-head performance comparison data against industry giants’ solutions | Request a white paper from the other party |
| Academic biotech exhibitors | Progress in the clinical translation of cutting-edge technologies | Availability of unpublished validation data to be shared after NDA submission | Exchange contact information → Stay updated on literature |
| CRO/CDMO | Global Central Laboratory Capabilities | Sample handling and cold chain logistics solutions in the Asia-Pacific region | Request a quote and SOP from the other party |
One detail that is often overlooked is that CDx collaboration discussions at ADLM are typically more efficient than those at ASCO or AACR. The reason is simple: ASCO attendees are primarily oncologists, who focus on clinical efficacy data; AACR attendees are primarily basic researchers, who focus on mechanisms of action.In contrast, ADLM attendees include a large number of decision-makers from pharmaceutical companies’ diagnostic collaboration departments—the very people responsible for CDx procurement and partnership agreements. Post-event survey data from ADLM 2025 shows that heads of diagnostic collaboration departments at exhibiting pharmaceutical companies conducted an average of 8.3 productive business meetings during the event, compared to just 3.1 for the same group at ASCO.This difference in efficiency stems from the nature of the events—ADLM is essentially a “diagnostic technology expo,” where attendees come with specific procurement needs, not to listen to presentations. Therefore, Chinese companies’ booth preparations at ADLM should focus on quantifiable technical parameters (sensitivity, specificity, TAT, throughput) rather than broad scientific narratives.
Finally, it is important to note that when selecting a CDx partner, one should not focus solely on the platform’s technical parameters but also assess whether the partner has experience in effectively communicating with regulatory authorities (particularly the FDA and EMA).A CDx partner with extensive experience in regulatory communication can help you establish a biomarker strategy aligned with regulatory expectations early in drug development, thereby avoiding major issues—such as inappropriate biomarker selection or unapproved assay methodologies—that could lead to project rework or even failure during Phase III clinical trials.At ADLM, you can gain a more intuitive understanding of the differences in regulatory compliance capabilities among various CDx companies by attending forums and workshops related to Regulatory Science.
4.0 Small-Molecule Targeted Therapies Session at the bio convention: Overcoming Drug Resistance and Guiding Precision Therapy Through Genetic Mutation Monitoring

4.1 Technological Frontiers: Monitoring “Drug-Resistance Gene Mutations” in Small-Molecule Drugs, Represented by TKI Inhibitors
4.1.1 Clinical Challenges: Mutant Gene Escape and Mechanisms of Drug Resistance Following Long-Term Use of Small-Molecule Drugs
Small-molecule targeted drugs—particularly tyrosine kinase inhibitors (TKIs)—have reshaped standard treatment regimens for multiple cancer types over the past two decades, including non-small cell lung cancer (NSCLC), chronic myeloid leukemia (CML), and gastrointestinal stromal tumors (GIST).Osimertinib (a third-generation EGFR-TKI) has achieved a median progression-free survival (mPFS) of 18.9 months in the first-line treatment of EGFR-mutated NSCLC—a figure that would have been unimaginable a decade ago.
But what happens after 18.9 months is where the real “battlefield” of oncology lies—drug resistance.The molecular mechanisms underlying osimertinib resistance have been thoroughly studied: the most common acquired resistance mutations are EGFR C797S (accounting for approximately 7–15% of patients with first-line resistance), MET amplification (approximately 15–20%), and histological transformation to small cell lung cancer (SCLC) (approximately 5–10%).The mechanisms underlying the remaining 50–60% of resistance cases have not yet been fully identified—some involve bypass activation (such as KRAS G12C and BRAF V600E), some involve epigenetic silencing, and some remain entirely unknown.
This “unknown” is one of the most frustrating aspects of clinical oncology—when a patient shows radiographic progression after 12 months of osimertinib treatment, the oncologist faces a critical decision-making window: should they continue osimertinib in combination with chemotherapy? Switch to another TKI? Or transition directly to immunotherapy?This decision-making “window” is typically 2–4 weeks—if we wait another 6–8 weeks for a tissue biopsy, genetic testing, and results, the patient’s PS score (performance status) may have already dropped from 0–1 to 2–3, losing the opportunity to switch regimens.
Liquid biopsy (ctDNA NGS) is currently the best tool for “rapidly deciphering resistance mechanisms.” Using just 10 mL of peripheral blood, a ctDNA mutation profile covering more than 50 genes can be obtained within 5–7 business days—without the need for a needle biopsy or waiting for pathology reports.However, liquid biopsy has its limitations: in patients with low tumor burden or where the tumor does not shed ctDNA (such as certain patients with brain metastases), the detection rate of ctDNA may be as low as 30–40%. Improving detection sensitivity and expanding the range of detectable mutations are the most active areas of R&D in the field of small-molecule resistance monitoring.
The EGFR C797S mutation is one of the most common mechanisms of resistance to third-generation EGFR TKIs (osimertinib), and there are currently no FDA-approved targeted therapies for this mutation. This means that patients face a treatment gap after developing C797S resistance, forcing clinicians to switch to chemotherapy or immunotherapy.However, a critical diagnostic challenge exists: the abundance of the C797S mutation in ctDNA is typically below 0.5% VAF. Traditional tissue biopsy-based NGS often misses this mutation due to sampling bias and detection limit constraints. In contrast, ultra-sensitive dPCR platforms can lower the detection limit for C797S to below 0.05% VAF, which is crucial for guiding subsequent treatment decisions for patients.At ADLM 2025, two Chinese dPCR companies showcased ultra-sensitive detection kits for EGFR C797S, attracting expressions of interest from multiple U.S. community oncology networks. This is a classic example of how breakthroughs in diagnostic technology directly create new clinical needs, thereby providing new patient stratification tools for drug development.
4.1.2 Evolution of Solutions: How Digital PCR (dPCR) and Next-Generation Sequencing (NGS) Technologies Enable Ultra-Sensitive Mutation Monitoring
In the field of mutation detection, dPCR and NGS represent two “complementary yet competing” technological approaches. Rather than repeating the standard sales pitches found in vendor brochures, let’s get down to the nitty-gritty.
The operational logic of dPCR (Digital PCR): A DNA sample is distributed into tens of thousands of microreaction units (droplets or chip wells), where each unit contains either 0 mutant molecules or ≥1.PCR amplification and fluorescence detection are then performed to count how many microreaction units are “positive,” and the number of mutant molecules in the original sample is calculated using a Poisson distribution. The key advantage of dPCR is absolute quantification—it requires no standard curve and no normalization against a reference gene, yielding a result of “how many mutant copies per milliliter of plasma.”In the monitoring of known mutation targets (such as EGFR T790M/C797S and KRAS G12C), the detection limit (LOD) of dPCR can reach 0.01% allele frequency—meaning that dPCR can detect a single mutant molecule among 10,000 normal DNA molecules.
The strength of NGS lies in its “breadth”—a single panel (such as the Illumina TSO 500) can simultaneously test all exonic regions of 523 genes, covering SNVs, indels, CNVs, gene fusions, and tumor mutational burden (TMB). However, the LOD for NGS is typically around 0.5–1.0%—1–2 orders of magnitude higher than that of dPCR.Why? Because the NGS library preparation process involves a PCR amplification step, which causes the signals of rare mutations to be “diluted”; furthermore, NGS itself has an inherent sequencing error rate of 0.1–0.5%, and mutation signals below this level are drowned out by sequencing noise.
Technical approaches to address the sensitivity limitations of NGS include unique molecular identifiers (UMIs)—tagging each original DNA molecule with a unique identifier, then using “consensus calling” to distinguish true mutations from errors introduced by PCR or sequencing.With UMI, the effective LOD of NGS can be improved from 0.5% to 0.05–0.1%—approaching that of dPCR, though a gap remains. Another approach involves targeted enrichment using “hybridization capture” rather than “amplicon” methods—the former exhibits less bias toward mutations, while the latter offers higher sensitivity but is limited to covering known target regions.
A key highlight of the dPCR vs. NGS debate at ADLM 2026 is that Bio-Rad is expected to showcase an upgrade to the multiplexing capabilities of its QX600 dPCR system, potentially expanding the number of targets detectable per well from two to six to eight.This will shift dPCR from a “one mutation per well” approach to “one well covering an entire resistance panel,” partially encroaching on the NGS market. Meanwhile, Illumina and Thermo Fisher will also showcase improvements in UMI and hybrid capture efficiency on their respective NGS platforms. If you are responsible for selecting clinical testing protocols, spending 30 minutes at the booths for both technologies to watch demos, ask about specifications, and request data will be far more effective than reading ten comparative literature articles.
Table 4.1: Comparison of Technical Parameters Between dPCR and NGS-UMI in Monitoring Resistance to Small-Molecule Targeted Therapies
| Performance Parameters | dPCR (Bio-Rad QX600) | NGS-UMI (Illumina TSO 500) | Clinical Applications |
| Limit of Detection (LOD) | 0.01–0.05% VAF | 0.05–0.1% VAF (UMI) | dPCR—Known resistance mutations; NGS—Broad-spectrum screening |
| Number of Targets per Test | 2–8 targets (2026 upgrade) | 523 genes, full exons | dPCR—Quantification of known mutations; NGS—Identification of unknown mutations |
| Absolute quantification | Yes (copies/μL) | No (relative VAF) | dPCR—Therapeutic Monitoring; NGS—Initial Diagnostic Pan-Panel |
| Sample requirement | 5–10 ng cfDNA | 20–50 ng cfDNA | dPCR is better suited for samples with low cfDNA yield |
| Turnaround Time (TAT) | 1–2 business days | 5–10 business days | dPCR—Urgent Clinical; NGS—Comprehensive Assessment |
| Cost per test | $200–400 per target | $1,500–3,000 per panel | dPCR—Single-target monitoring; NGS—Initial screening |
4.2 The Showdown at the ADLM Exhibition Hall: The Commercial Evolution of Liquid Biopsy and Ultra-Sensitive Testing Devices
4.2.1 Hardware and Algorithm Innovations in Molecular Diagnostics by Global Giants and Innovative Biotech Companies
The molecular diagnostics exhibition area at ADLM (typically located in Halls B and C of the Anaheim Convention Center) is the most fiercely competitive section of the event each year. It serves as the “technological high ground” of the entire exhibition—whichever company secures the largest booth space and showcases the latest equipment here will dominate industry discourse for the next 12 months. In 2026, the following trends warrant particular attention:
First, competition for fully automated “one-click NGS” solutions is intensifying. Illumina’s NovaSeq X series and Thermo Fisher’s Genexus system are both pursuing “sample-to-report” full automation—operators simply load plasma samples into the instrument, press a button, and view mutation reports directly on the screen within 24–48 hours.This “one-click” convenience comes at a significant cost—the instruments themselves typically range from $300,000 to $800,000, with reagent and consumable costs of $1,500–$3,000 per sample. However, for a clinical center requiring large-scale ctDNA screening, this investment can be amortized within 3–5 years.
Second, AI-assisted variant calling and annotation is shifting from a “nice-to-have” to a “standard feature.” Prior to 2024, sequencing instrument vendors competed on “hardware specifications”—read length in base pairs, throughput in gigabases, and accuracy metrics like Q30/Q40.By 2026, hardware specifications will no longer be a significant differentiator, and the focus of competition has shifted to bioinformatics algorithms and AI interpretation. Illumina’s DRAGEN platform, Thermo’s Ion Reporter, and a number of independent AI companies (such as PathAI and Paige.AI) all showcased performance improvements in rare variant detection, fusion gene identification, and TMB calculation at ADLM.
Third, the rise of the “Multi-Omics” exhibition zone. In 2026, ADLM introduced a new section called the “Multi-Omics Integration Zone”—a somewhat tongue-twisting name, but essentially it means integrating genomics (DNA-seq), transcriptomics (RNA-seq), and proteomics (LC-MS/MS) data onto a single platform for cross-analysis.For small-molecule resistance monitoring, this means you can not only see that “the EGFR C797S mutation has appeared,” but also determine simultaneously whether “this mutation is activated at the transcriptional level or epigenetically silenced”—the latter determines whether you should subsequently use a TKI in combination with an epigenetic drug (such as an HDAC inhibitor) or switch directly to a different TKI.
Competition among international giants in the molecular diagnostics hardware sector has shifted from a simple comparison of technical specifications to the development of ecosystem solutions.Companies such as Illumina, Thermo Fisher, Roche, and Qiagen no longer merely sell instruments and reagents; instead, they have built comprehensive solutions covering sample preparation, library construction, sequencing/detection, data analysis, and report generation. This implies that the competitive advantage of individual technical components is diminishing—buyers now place greater emphasis on the integration and interoperability of the entire workflow.For innovative companies in the ADLM sector, the path to competing with giants does not lie in surpassing them on a single metric, but in identifying a specific clinical application scenario where they can offer a specialized solution that is more efficient and cost-effective than the giants’ generic offerings. This “single-point breakthrough” strategy has been proven successful multiple times in the history of ADLM—both Guardant Health and Foundation Medicine entered the market by targeting a specific testing scenario and eventually grew into independent companies valued at billions of dollars.
4.2.2 From Sample to Answer: How to Lower the Barriers to Implementing Precision Medicine in Frontline Clinical Practice
Small-molecule drug resistance monitoring is already quite well-established in academic medical centers (such as MD Anderson, MSKCC, and Peking University Cancer Hospital)—these institutions have dedicated Molecular Tumor Boards, bioinformatics teams, and sufficient budgets to send samples for NGS. But the crux of the problem lies elsewhere—90% of cancer patients are not treated at academic medical centers; they are treated in oncology departments in prefecture-level cities or outpatient oncology clinics at county hospitals.In these settings: there is no NGS equipment, no bioinformatics team, and sending a sample to a third-party company for NGS takes 2–3 weeks; primary-care physicians are not equipped to interpret complex genetic reports.
This is precisely why the “Sample-to-Answer” all-in-one system exists. The goal of such devices is not to replace the breadth of NGS, but to achieve “extremely fast, extremely simple, and extremely affordable” mutation detection within a “limited gene set.” A typical application scenario is as follows: A patient with advanced NSCLC returns for a follow-up visit at the oncology department of a county hospital, where imaging reveals disease progression.The doctor draws a blood sample, places it in a benchtop dPCR all-in-one system, and within an hour, the screen displays: EGFR T790M—negative; MET amplification—positive. The doctor immediately decides to prescribe a MET inhibitor (such as sevotinib or camtinib), without needing to wait two weeks for an NGS report from an external testing company—the patient’s condition cannot wait that long.
Notable “Sample-to-Answer” products to watch at ADLM 2026 include: Cepheid’s GeneXpert system—this platform is already the global standard for drug-resistant tuberculosis testing and is now expanding into tumor mutation profiling.BioMérieux’s BioFire FilmArray—which dominates the field of molecular diagnostics for infectious diseases—with oncology as its next target market. And a wave of emerging “microfluidics + dPCR integrated” startups—their devices are typically only the size of a microwave oven, with a per-test cost of $50–100. Their goal is not to outperform NGS in technical specifications, but to enable primary care hospitals to “afford it, perform it quickly, and perform it accurately.”
For Chinese medical device companies expanding overseas, the “sample-to-answer” approach presents an extremely attractive entry opportunity. China’s supply chain maturity in microfluidics and POCT molecular diagnostic devices is already high, while the “gap in primary care testing capabilities” at primary care hospitals in Europe and the U.S. is equally significant. ADLM 2026 will be an excellent showcase for Chinese companies to demonstrate “cost-effectiveness and ease of use” in the molecular diagnostics field.
Table 4.2: Matrix of Sample-to-Answer Capabilities and Applicable Scenarios for Small-Molecule Drug Resistance Monitoring Devices
| Product/Platform | Technology Type | Range of Detection Targets | TAT | Equipment Price (USD) | Applications |
| Cepheid GeneXpert | Real-time Fluorescent PCR | 1–8 targets per run | 30–120 min | $15–30K (equipment) | Rapid single-mutation detection / Primary care |
| BioFire FilmArray | Multiplex nested PCR | 20–30 targets/panel | ~60 min | $25–40K (equipment) | Multi-target syndrome panel/emergency |
| Bio-Rad QX600 | Digital PCR | 2–8 targets (2026) | 2–4 hours | $80–120K (equipment) | High-sensitivity quantification/therapeutic monitoring |
| Oxford Nanopore MinION | Nanopore sequencing | Whole-genome (low coverage) | 1–4 hours | $1–3K (equipment) | Rapid Whole-Genome Overview/Structural Variations |
| NGS Outsourcing (F1CDx) | Hybridization capture NGS | 324-gene whole-exome | 10–14 days | $3,500–5,800 per test | Comprehensive Genomic Analysis / Academic Center |
BTK inhibitors also have a unique mechanism of resistance—the BTK C481S binding site mutation. This mutation directly prevents ibrutinib from covalently binding to the active site of BTK, resulting in complete acquired resistance.The most sensitive method for detecting the BTK C481S mutation is dPCR—in the plasma ctDNA of CLL patients, the allele frequency of the BTK C481S mutation is typically only 0.1–1.0%, which falls precisely within the optimal detection range of dPCR.This is why physicians in the B-cell oncology department are frantically searching for the most sensitive dPCR platform at ADLM—their patients are waiting to switch to non-covalent BTK inhibitors (such as pirtobrutinib), and the key evidence for the switch decision hinges on that 0.1% mutation signal.
Take chronic lymphocytic leukemia (CLL) as an example: after patients take BTK inhibitors (such as ibrutinib or acatitinib), a significant proportion of patients achieve an “undetectable MRD” (uMRD) status in peripheral blood.But the question is—are current MRD detection standards (multiparameter flow cytometry, with a sensitivity of ~10⁻⁴, or one in ten thousand) sufficient? Studies show that among CLL patients who test “negative” by flow cytometry, approximately 40% still have detectable ultra-low levels of residual clones when using NGS-based IgH rearrangement clonotypic tracking.This implies that—even when you believe a patient is “completely clear,” they may not actually be. At the 2026 ADLM conference, Adaptive Biotechnologies’ clonoSEQ platform and Invivoscribe’s LymphoTrack panel are both pushing the limits of MRD detection sensitivity—advancing from 10⁻⁴ toward 10⁻⁶ (one in a million).
Discussions on resistance monitoring for small-molecule targeted therapies typically default to the context of solid tumors—lung cancer, breast cancer, and colorectal cancer.However, monitoring of measurable residual disease (MRD) in hematologic malignancies (leukemia, lymphoma, and myeloma) is becoming the most dynamic market where small-molecule targeted therapies (particularly BTK inhibitors, FLT3 inhibitors, and IDH1/2 inhibitors) intersect with liquid biopsy technology.
The commercialization progress of Sample-to-Answer platforms directly determines the speed at which small-molecule targeted therapies are implemented in clinical practice. When a lung cancer patient with an EGFR T790M mutation needs to switch from osimertinib to omertinib, clinicians cannot wait a week for an NGS report from an external laboratory—they need results within 24 hours. This is the raison d’être of Sample-to-Answer platforms.Currently, there are only six FDA-approved Sample-to-Answer platforms for cancer genetic testing, while clinical demand spans over 200 mutation profiles. This gap represents an opportunity for innovative companies at the ADLM exhibition.
4.3 Practical Guide to Visiting and Attending the Exhibition (Small Molecule Track)
4.3.1 Types of Booths Worth Visiting: IVD Solution Providers with High-Throughput, Ultra-Sensitive Mutation Detection Capabilities
The approach to visiting exhibits in the small-molecule resistance monitoring sector differs from that of the large-molecule track. While the large-molecule track focuses on “whether a target is present,” the small-molecule track focuses on “when a mutation appears”—one is static detection, the other is dynamic monitoring. Therefore, when selecting booths, prioritize companies that offer “longitudinal tracking” solutions. Specific screening criteria:
① Check if they have a “patient-level” mutation tracking database—one that doesn’t just provide a mutation list after a single test, but can compare a patient’s ctDNA mutation profiles at different time points to generate a “molecular progression trajectory.” Guardant Health’s Guardant360 and GuardantReveal are designed around this concept, and Foundation Medicine also offers similar longitudinal monitoring solutions.
② Examine their limit of detection (LOD) and quantitative accuracy. Ask exhibitors at the booth: “For the specific EGFR T790M site, what are your detection limit and quantitative linear range?”—True experts will quote specific numbers; if a salesperson says “our sensitivity is very high,” politely take your leave.
③ Check if they have publicly documented collaborations with pharmaceutical companies. If an NGS/dPCR company has provided “companion diagnostic + resistance monitoring” services for a Phase III clinical trial by Roche, Novartis, or AstraZeneca, its SOPs and quality systems are trustworthy—because pharmaceutical companies’ clinical quality control standards are even stricter than FDA laboratory certifications (CLIA/CAP).
4.3.2 How Attendees Should Evaluate These Technologies: The Commercial Trade-offs Between Stability, Testing Costs, and Turnaround Time
After reviewing 10 sequencing companies, 5 dPCR manufacturers, and 3 Sample-to-Answer systems at ADLM—how do you choose? You need a “three-dimensional evaluation framework”:
Dimension One—Analytical Stability. If the same sample is split into three portions and sent to the same company’s labs in the U.S., Europe, and China, what is the concordance rate among the three reports? The industry-recognized standard for “excellent” performance is ≥95%. If a vendor cannot provide multi-center concordance data, or if the data consists only of “internal validation” without “external independent validation”—proceed with caution.
Dimension 2—Per-Test Cost. Note that this refers not to the “list price,” but to the “actual on-site cost”—the total cost encompassing instrument depreciation, reagents and consumables, bioinformatics analysis, labor costs, and time costs.A complete NGS panel may fall within a total cost range of $2,000–5,000 per test; a single-target dPCR test ranges from $150–400 per test; and a Sample-to-Answer integrated system ranges from $50–200 per test.Your required testing frequency determines your total budget—if a patient’s resistance monitoring requires testing every two months for two years, that amounts to 12 tests—choosing dPCR or a sample-to-answer system results in a TCO (Total Cost of Ownership) that is one order of magnitude lower than choosing NGS.
Dimension Three—Turnaround Time (TAT). This is the most overlooked dimension, yet it has the greatest clinical impact. An NGS report typically takes 10–14 business days from sample shipment to receiving the PDF; an in-house dPCR test takes 1–2 business days; and a Sample-to-Answer integrated system takes 1–4 hours.In the context of community hospitals, the difference in TAT represents the chasm between “whether a patient can adjust their treatment plan on the same day of their visit” and “whether a patient must wait two weeks for results.” This is not a matter of efficiency—it is a matter of the patient’s life expectancy.
When evaluating technologies at ADLM, don’t let booth designs and giveaways distract you. Gather data on these three dimensions—stability, cost, and TAT—and compile them into a single Excel spreadsheet for side-by-side comparison.Then take the spreadsheet to the evening forum reception, find other attendees who have used these platforms (most of them will be wearing white coats and “Speaker” name tags), and ask: “What has your center’s actual experience been like? Have you encountered instrument downtime or significant batch-to-batch variability?”—This is the final and most critical piece of evaluation data you’ll obtain: real-world user experience.
Table 4.3: Three-Dimensional Evaluation Framework and Standards for Small-Molecule Drug Resistance Monitoring Technologies at ADLM
| Evaluation Dimensions | Specific Parameters | Acceptable Standard | Excellent Standard |
| Analytical Stability | Multicenter Concordance | ≥90% | ≥95% |
| Detection Sensitivity | LOD at the locus level (VAF%) | <0.5% VAF | <0.1% VAF |
| Cost per test | Total Cost of Ownership (TCO) | $500–1,000 (dPCR) | $100–300 (sample-to-answer) |
| Turnaround Time (TAT) | Sample-to-Report Time | 3–5 business days (NGS) | 1–2 business days (dPCR)/<4 hours (all-in-one system) |
| Pharmaceutical Company Collaboration Cases | Companion Diagnostics Experience | ≥2 biotech companies | ≥1 top-20 pharmaceutical company |
For small-molecule targeted drug companies, ADLM is not a trade show for selling drugs. However, it is an excellent platform for showcasing the logic behind precision medicine.An increasing number of Chinese small-molecule innovative drug companies are adopting a “drug + CDx” co-presentation strategy at ADLM—displaying the MOA (mechanism of action) diagram of a drug candidate alongside the corresponding companion diagnostic kit. This sends a clear signal to potential partners: the target patient population for this drug has been precisely defined, which will significantly improve clinical trial enrollment efficiency.This presentation strategy was successfully validated at the 2025 ADLM by two Chinese companies developing KRAS G12C inhibitors, attracting expressions of interest from multiple U.S. community oncology networks.
When evaluating testing platforms, one criterion often overlooked by many Chinese exhibitors is the status of fundamental performance validation. When introducing a new testing platform, U.S. CLIA laboratories do not prioritize sensitivity data—which represents ideal conditions provided by manufacturers. Instead, they examine parallel validation reports from multiple independent CLIA laboratories—particularly reproducibility data in scenarios involving low-frequency mutations (<1% VAF).If your booth lacks this data, CLIA laboratories will not consider your platform, even if its sensitivity parameters are superior. We recommend that exhibitors prepare a concise “Validation Summary Card” for their booth—a single-page document listing key performance comparison data from at least three CLIA laboratories. This tool is far more effective at ADLM than any printed material.
Another often-overlooked yet critical dimension when evaluating diagnostic technologies at the exhibition is “the actual impact of turnaround time (TAT) on clinical decision-making.”In the clinical setting of targeted cancer therapy, if the TAT from sample receipt to the delivery of actionable mutation test results exceeds seven days, clinicians often no longer have time to wait—they are forced to initiate empirical treatment based on experience, which runs counter to the very purpose of precision medicine.Therefore, when speaking with equipment suppliers at ADLM, TAT should be treated as a mandatory metric: How long does it take from sample entry into the device to the issuance of a complete report? Does this timeframe include the bioinformatics analysis phase? Will this time significantly increase when sample volume doubles during peak periods? The answers to these questions often reflect a platform’s actual clinical usability far more accurately than the sensitivity figures listed in technical specifications.
5.0 Business Insights from the bio convention: The “Reverse Survival Logic” and Overseas Business Opportunities Behind the 20,000+ Attendee Mega-Exhibition
5.1 Why is 2026 considered a pivotal year for nucleic acid and bio-diagnostics companies to “reduce costs and improve efficiency”?
5.1.1 The Face-to-Face Psychological Game Between Global Buyers and Sellers: Seeking “High-Value-for-Money” Raw Materials in a Highly Competitive Market
If you’ve attended any international conference related to the biopharmaceutical supply chain over the past three years, you’ve likely sensed the growing “price anxiety” in the air. During the pandemic in 2021–2022, the seller’s market for nucleic acid raw materials gave suppliers pricing power—prices for plasmids, modified nucleotides, and enzymes soared to levels no one could have imagined in 2019.In 2023–2024, the market began to “normalize,” but prices did not return to pre-pandemic levels—suppliers had grown accustomed to high profit margins, and customers had been forced to accept that “this is simply the going rate in the industry.”
2026 is different. The global biopharmaceutical financing environment has tightened—PitchBook data shows that the number of biotech IPOs in Q1 2026 hit its lowest level for that quarter since 2016—meaning biotech companies have less cash on hand than before and are more sensitive to upstream costs.At the same time, GMP production capacity built by raw material suppliers in China and India over the past two years is beginning to come online on a massive scale—global total production capacity for modified nucleotides has grown by nearly 60% compared to 2023. This reversal in the supply-demand dynamic is shifting the nucleic acid raw materials market from a “seller’s market” to a “buyer’s market.”
The Clinical Lab Expo at ADLM 2026 is the first major battleground of this “buyer’s market.” The same scene is playing out at every booth: buyers are comparing quotes from three different suppliers, shuttling between booths to negotiate prices.Suppliers’ VPs of Sales are facing unprecedented pressure—they know that if their quote is 10% higher, the buyer might simply walk 20 meters to a competitor’s booth and sign a deal at a price 10% lower.
This is good news for buyers, but there’s a catch—”cheap” doesn’t equal “good value.” In the field of nucleic acid raw materials, ingredients that are “cheap but have high batch-to-batch variability” are ticking time bombs:If you use it to produce three batches of mRNA drugs—with the first batch yielding 100% expression, the second 85%, and the third 60%—the FDA will demand an explanation, and the cost of that explanation will far exceed the initial savings from the lower material price. When making procurement decisions at ADLM, the key is not to find the cheapest supplier, but to find “the cheapest supplier that meets your acceptable quality threshold.”You must define this threshold yourself—take the supplier’s COA and compare it with your process development report to identify 3–5 “non-negotiable” quality parameters (such as modified NTP purity ≥99.5% or T7 polymerase RNase residue ≤ detection limit), and then only compare prices for suppliers that meet or exceed these standards.
A practical tip: At the ADLM booth, display raw material samples organized by application rather than by product catalog. Traditional booth layouts are typically “product line-oriented”—with all enzyme preparations in one area and all nucleotides in another. However, U.S. buyers think in a “project-oriented” way—they come to ADLM to source raw materials for a specific project.If your booth is organized by application (e.g., “mRNA drug development kits,” “NGS panel library preparation kits,” “CDx quality control reference material sets”), buyers will be able to locate the product lines they need more quickly.Post-show survey data from ADLM 2025 shows that booths organized by application scenario saw 40% longer buyer dwell times and 60% higher inquiry rates compared to booths organized by product line.
The global nucleic acid raw material market is undergoing a major shakeup in 2025–2026. Three driving factors are at play simultaneously: supply chain restructuring pressures from the Biosecure Act, a surge in demand for modified nucleic acids driven by the explosion of mRNA therapies, and shrinking margins on sequencing reagents due to price wars in NGS panels. For Chinese nucleic acid raw material suppliers, the impact of these three trends is mixed.The pressure from the Biosecure Act primarily affects raw material trade exported directly from China to the U.S., but for companies that have established overseas production capacity and compliance systems through third countries (such as Singapore and Ireland), this may actually present an opportunity—as some competitors may exit the market due to excessively high compliance costs.The boom in mRNA therapeutics directly benefits suppliers with the capability to synthesize modified nucleotides (such as pseudouridine-modified nucleotides), as this market is projected to grow by over 300% between 2024 and 2026.Conversely, the impact of the NGS price war is relatively negative, as an increasing number of pharmaceutical companies are in-sourcing NGS testing, reducing their reliance on third-party reagents. The convergence of these three trends means that when showcasing your raw materials at ADLM, you can no longer rely on the generic pitch of “our quality is excellent and our prices are low”; instead, you must provide a differentiated value proposition tailored to each specific application scenario.
5.1.2 Latest Requirements in Major European and U.S. Markets Regarding Supplier Qualifications and Compliance (e.g., New FDA Regulations, LDT Regulatory Trends)
When expanding into the global diagnostics and raw materials market in 2026, compliance is not an optional choice—it is a prerequisite for doing business. Below are the most noteworthy compliance developments to watch during ADLM 2026:
First, the FDA is tightening its regulation of LDTs (Laboratory-Developed Tests). In May 2024, the FDA issued a Final Rule formally incorporating LDTs into the medical device regulatory framework, to be implemented in phases: Phase One (May 2025) requires LDTs to comply with Medical Device Adverse Event Reporting (MDR) requirements; Phase Two (May 2026) requires compliance with Registration and Listing;Phase 3 (May 2027) will require compliance with a full quality system (QSR/GMP). This means that if your company sells “Research Use Only” (RUO) reagents to the U.S. for clinical decision-making, and your customers use these RUO reagents for LDT testing—both parties are operating in a gray area, and the window of opportunity is closing.
Second, the pressure of the full implementation of the European IVDR (In Vitro Diagnostic Medical Devices Regulation). IVDR 2017/746 officially took effect in May 2022, but granted different transition periods for products of varying risk levels. By 2026, the transition periods for all high-risk (Class C and Class D) IVD products will have expired.Any high-risk IVD product that has not obtained the IVDR CE mark will no longer be permitted to be sold on the EU market. This represents a massive shock for Chinese IVD companies expanding overseas—many products that previously obtained CE marking under the old IVDD directive must be re-submitted in accordance with the IVDR, and the IVDR’s requirements are far stricter than those of the IVDD (particularly regarding clinical evidence and post-market surveillance).
Third, supply chain security and the trend toward “friend-shoring.” The geopolitical landscape in 2026 is reshaping the layout of the biopharmaceutical supply chain. The U.S. and the EU are using policy tools—such as the U.S. Biosecure Act draft and the EU’s Critical Medicines Act—to encourage pharmaceutical and diagnostic companies to “reshoring” or “nearshoring” the production of critical raw materials to so-called “trusted countries.”For Chinese API suppliers, this means you must demonstrate not only “price advantages” but also “international recognition of your quality system” on ADLM—has your facility passed an FDA on-site inspection? Do your quality documents comply with ICH Q7 (API GMP)? Are you willing to open your facility to third-party audits by overseas clients? The answers to these questions determine whether buyers classify you as a “strategic supplier” or a “temporary substitute.”
Table 5.1: Key Compliance Focus Areas for Biodiagnostics and API Suppliers Expanding Overseas in 2026
| Compliance Dimensions | Key Regulations/Policies | Effective Date | Impact on Chinese Companies Expanding Overseas |
| FDA Regulation of LDTs | FDA Final Rule (LDTs as Medical Devices) | Phase 2: May 2026 (Registration Listing) | Path from RUO Reagents to LDTs is restricted; IVD pathway must be planned in advance |
| European IVDR | Regulation (EU) 2017/746 | Class C/D Transition Period Deadline: 2026–2027 | Existing CE certificates must be re-notified under the IVDR, resulting in increased costs |
| Supply Chain Security | Biosecure Act/Critical Medicines Act | Draft stage, ongoing development | Must demonstrate international recognition of the quality management system; third-party audits permitted |
| Data Integrity | FDA 21 CFR Part 11/EU Annex 11 | Ongoing enforcement | Electronic records and electronic signatures must be compliant; QC data must be tamper-proof |
| GDPR/Data Privacy | EU GDPR/State Privacy Laws (US) | Ongoing Enforcement | Cross-border transfer of genetic data requires a pre-established compliance plan |
“Going global” isn’t just about selling products—it’s about selling services, selling expertise, and selling the fact that “we understand the FDA.”You need a team capable of engaging with U.S. biotech clinical development teams on the same technical level—one that doesn’t say, “Our prices are 30% lower,” but rather, “We’ve supported 7 IND filings with CDx components over the past 2 years, and 5 of them received FDA clearance within 30 days without any clinical holds related to the CDx section.” Behind this messaging lies tangible regulatory experience and a track record of success.At ADLM 2026, one trend worth paying special attention to is whether any Chinese diagnostic companies will begin showcasing their FDA-approved CDx cases at their booths. If so, that will mark a milestone moment for the Chinese diagnostic industry as it transitions from “OEM manufacturing” to “brand globalization.”
At ADLM 2026, China’s IVD and diagnostics companies face a critical strategic choice: continue with “exporting raw materials” (selling plasmids, enzymes, and modified nucleotides to European and American clients), or upgrade to “exporting solutions” (selling complete companion diagnostic development services, or even CDx co-development partnerships).The gross margin for the former ranges from 20% to 40%, while that for the latter ranges from 50% to 70%—but the barriers to entry for the latter rise exponentially.
For Chinese companies planning to seek European and American regulatory compliance partners at ADLM, a practical tip is to prepare a “compliance checklist” in advance. This document doesn’t need to be complex—a single page is sufficient—listing the current certification status of your product in major markets, existing gaps, and a timeline for addressing them.Compliance consultants in the U.S. and Europe won’t spend time explaining regulatory frameworks to you—they’re already well-versed in their own systems. What they want to know is: Have you started your compliance preparations? Which steps are missing? And what is your timeline? Companies that can clearly answer these questions at the booth typically receive more follow-up opportunities after the exhibition.
For companies expanding overseas, the most significant compliance changes in 2026 will occur within two regulatory systems. In the U.S., the FDA’s LDT final rule will officially take effect in Q3 2026, meaning all laboratories providing LDT services in the U.S. market must complete their compliance transition within the specified timeframe. The impact on Chinese IVD companies is indirect: many U.S. laboratories will seek FDA-approved alternatives during the transition period, creating a window of opportunity.In the EU, pressure from the IVDR transition period is forcing European buyers to accelerate the shift from products with the old CE marking to those with the new IVDR certification. This means that showcasing CDx products with IVDR certification at ADLM will be more competitive than ever before.
5.2 Cross-Border Collaboration and Localized Thinking: How to Conduct Business Negotiations Using the Language of U.S. Healthcare Professionals
5.2.1 Avoid “Chinesized English” Thinking: Emphasize “Clinical Compliance, Supply Chain Stability, and Technological Iteration Capabilities” in Technical Pitching and Product Demonstrations
If you walk through the ADLM exhibition hall, you’ll hear English spoken with a variety of accents—American, British, Indian, German, Japanese, and Chinese. But “accent” isn’t the problem; “mindset” is.The most common business communication mistake made by Chinese companies expanding overseas isn’t grammatical errors, but a “mismatch” in value propositions—you’re desperately emphasizing things the buyer doesn’t care about, while failing to mention the very points that matter to them.
Specifically, Chinese suppliers often open conversations at their booths with these four phrases:
① “Our prices are 30–50% lower than market rates.” (This statement immediately raises two questions for American buyers: Why so cheap? Is there a compromise on quality?)
② “We are China’s largest producer of XX raw materials.” (U.S. buyers aren’t impressed by “largest”—they want to know whose pipeline your product has already been used in)
③ “We can customize according to your needs.” (This statement conveys zero information—customization capabilities in the supply chain are a basic expectation, not a competitive advantage.)
④ “Our quality system is ISO 9001 certified.” (ISO 9001 is the most basic, generic quality certification; in the pharmaceutical industry, it’s a “entry-level” requirement, not a “competitive advantage.” You should tell them that you’ve passed the FDA’s PAI (Pre-Approval Inspection), or that your facility has been audited by a global Top 10 pharmaceutical company and added to their list of qualified suppliers.)
The three priorities that U.S. buyers truly care about are: ① Can your quality system ensure I won’t face challenges from the FDA when submitting an IND/NDA? ② Can your supply capacity scale up in tandem as I expand from Phase II to Phase III and then to commercialization? ③ Is your price competitive at the “same quality level”? — Note that price ranks third, and there is an important qualifying condition preceding it: “same quality level.”
Therefore, your 30-second elevator pitch at the booth should be structured as follows: First sentence: “We supply GMP-grade modified nucleotides for XX Pharmaceutical’s XX ADC drug pipeline and have passed the company’s supplier quality audit.” Second sentence: “Our GMP facility in Suzhou has an annual production capacity of XX kilograms and can scale up to XX kilograms within six months, supporting full-cycle supply from IND through commercialization.””Third sentence: “Our prices are 15–25% lower than those of U.S. suppliers at the same quality level—this is based on data from three head-to-head quality comparison tests we’ve passed.”—These three sentences respectively address quality endorsement, supply capacity, and price competitiveness, with not a single word of fluff.
The core principle for avoiding “Chinesed English” in technical roadshows is: let the data speak, drive the narrative with real-world scenarios, and build trust through a chain of evidence. Specifically, Chinese companies should pay attention to the following details when preparing for their booths. First, all booth materials (posters, brochures, technical data sheets) must be reviewed by a native English speaker.This is not a matter of “translation quality,” but rather a matter of “technical communication style”—Chinese technical writing tends to be comprehensive and exhaustive, while English technical communication places greater emphasis on highlighting key information and being action-oriented. Second, prepare 3–5 standardized case studies, each containing: client background, challenges faced, solutions provided, and quantifiable results.One of the most trusted sources of information for U.S. biotech procurement decision-makers is peer experience—if your case studies mention peer companies they recognize, conversion rates will increase significantly. Third, booth staff’s English communication skills must extend beyond technical terminology—they need to be able to conduct business conversations fluently, including discussions on pricing, delivery timelines, technical support, and after-sales service terms.
5.2.2 On-Site Networking Tips: How to Quickly Break into Core Technology Circles in Anaheim
In Anaheim, “building relationships” is more important than “doing business”—because real deals aren’t closed at the booth, but finalized at social events outside the exhibition hall. Here are practical strategies for quickly establishing effective connections at ADLM:
First, target the “evening golden window”—every day from 5:00 PM to 7:30 PM. During this time, the exhibition halls are closed, but major exhibitors host invitation-only receptions at hotels adjacent to the convention center (Anaheim Marriott, Hilton Anaheim).The barriers to entry for these receptions are low—in most cases, you simply need to register in advance on the exhibitor’s website or pick up an invitation card from a staff member at their booth on the day of the event. Having a beer and spending 15 minutes discussing technical pain points with the CSO of that CDx company you’ve been eyeing for two days is far more valuable than waiting in line for 10 minutes at the booth to shake hands with the VP of Sales.
Second, make good use of “hometown associations” and “alumni networks.” Anaheim is located in the Los Angeles metropolitan area—a hub for Chinese professionals in the biopharmaceutical industry on the U.S. West Coast.Every year during ADLM, the Southern California Chinese Biomedical Association (SCCBA) and several alumni associations of Chinese international students (from Peking University, Tsinghua University, Fudan University, Shanghai Jiao Tong University, etc.) organize in-person dinners or small seminars. A natural “foundation of trust” exists in these settings—a shared alumni identity is more effective than a hundred business cards.
Third, “Turning Academic Sessions into Social Opportunities”—this is the most underrated networking strategy. After an academic session on the second floor concludes—especially those specialized sessions with only 30–50 attendees—don’t leave immediately. Walk up to the podium, chat with the speaker for two minutes, and ask a specific technical question (not just a generic “great talk”).Speakers—especially those in academia—naturally appreciate attendees who genuinely understand their work. After two minutes of academic discussion, ask naturally: “Are you going to the reception tonight? I’d love to continue this conversation.” If this approach works, the connection you establish will be deep and grounded in technical trust—far surpassing what you’d gain by scanning a QR code to add someone on LinkedIn.
Fourth, don’t rely too heavily on interpreters. At U.S. conferences, if you bring an interpreter to talk with a foreigner, will the other person instinctively focus on you or the interpreter? The answer is “whomever is speaking”—but the content delivered by a Chinese interpreter often contains inaccuracies in technical terminology.If your English isn’t fluent, that’s no excuse to avoid networking—prepare three English scripts in advance (a 30-second self-introduction, a 2-minute technical overview, and a 5-minute partnership proposal), and practice them repeatedly until you can deliver them naturally. At a trade show, speaking English with an accent but delivering professional content is far more effective than relying on a translator and diluting your message.
Table 5.2: ADLM 2026 On-Site Networking Scenarios and Strategy Matrix
| Social Scenario | Best Time | Target Audience | Core Strategy | Behaviors to Avoid |
| Exhibitor Reception | Daily from 5:00 PM to 7:30 PM | Exhibitor executives, application scientists | Obtain an invitation card in advance; discuss specific technical challenges | Forcibly handing out business cards, discussing only price |
| Alumni/Hometown Reunions | Evening 8:00 PM–10:00 PM | Chinese professionals, scientists returning from abroad | Build technical trust first, then naturally transition to collaboration | Pushing products right off the bat |
| Networking after the academic session | 15 minutes after the session ends | Speakers (keynotes), academic KOLs | Ask specific technical questions to demonstrate in-depth understanding | Superficial compliments |
| Chance encounters in the exhibition hall | Randomly throughout the day | Anyone wearing a “Speaker” badge | Strike up a natural conversation, starting with a shared industry topic | Cold Pitch |
| Pre-event outreach on LinkedIn | 2 weeks before the meeting | Target companies and individuals | Send personalized invitations, mentioning shared interests | Bulk template messages |
Third, complete buyer outreach 30 days in advance. Do not wait until the week before the event to start emailing potential clients. Starting June 26, 2026 (30 days before the event), launch the ADLM Buyer Outreach Program—use LinkedIn Sales Navigator to identify VPs of Procurement and R&D at pharmaceutical companies confirmed to attend, send personalized one-on-one invitation emails, and schedule 15-minute in-person meetings during the event.Fourth, clearly define booth responsibilities. A common mistake is having the Sales Director handle product presentations, collect business cards, and monitor the exhibition app for inquiries all at once. Assigning roles to three people ensures efficiency: one product expert handles technical explanations and demo presentations; one business liaison collects business cards and schedules post-show one-on-one meetings; and one intelligence gatherer focuses on collecting market intelligence from competitors’ booths and forum sessions.
Based on the above analysis, for Chinese IVD and biopharmaceutical companies planning to exhibit at ADLM 2026, the following practical booth recommendations are derived from on-site observations of the three ADLM editions from 2023 to 2025 and feedback from surveys of U.S. biopharmaceutical procurement managers.First, booth location is more important than booth size. The ADLM exhibition space exceeds 400,000 square feet, and foot traffic in the North Hall and South Hall can differ by a factor of three or more. If your budget is limited, choose a small booth on a main aisle in the South Hall rather than a large booth in a corner of the North Hall. Second, demos are more effective than brochures.The most common refrain from U.S. biotech procurement managers is, “Show me the data, don’t tell me the story.” Bringing a live analytical instrument, a real-time data display screen, or at least an interactive LIMS system demo on an iPad is far more persuasive than any beautifully printed brochure.
A more advanced strategy is a “scenario-based demo”—focusing not on technical details, but on simulating the client’s actual workflow. For example, you could open with: “Suppose you’re a biotech company developing a KRAS G12C inhibitor, and your Phase III clinical trial requires confirming patients’ KRAS G12C mutation status at enrollment. You currently use an external NGS lab with an average turnaround time (TAT) of 14 days and a cost of $800 per patient.Our dPCR platform can reduce TAT to 2 days and lower costs to $200, while achieving a sensitivity of 0.1% VAF in low-frequency mutation scenarios.” The power of this scenario-based pitch lies in the fact that it allows the buyer to directly see how your product adds value to their work. Compared to abstract comparisons of technical specifications, scenario-based pitches typically yield 2–3 times higher conversion rates.
A common mistake during technical presentations at ADLM is overemphasizing “how advanced our technology is.” When U.S. biotech procurement decision-makers hear this, their internal reaction is usually: “So what? Show me the data.” They aren’t concerned with technological sophistication, but rather three specific questions: First, can your testing solution be directly applied in my clinical setting? Second, does your TAT (turnaround time) meet my clinical decision-making window?Third, do you have the necessary regulatory approvals in my target market? If you can answer these three questions in three minutes and provide concrete data, your success rate in negotiations will significantly increase.
A practical pre-exhibition preparation tool is a standardized template for a “one-minute elevator pitch.” Every booth representative should be able to answer three questions within 60 seconds: Who we are, what we do, and why you should care.It sounds simple, but in practice, most Chinese companies make a common mistake during these 60 seconds—spending too much time on “Who we are” (company profile, size, history) and too little on “Why you should care” (specific value to the buyer).The recommended breakdown is: 10 seconds on “Who we are,” 15 seconds on “What we do,” and 35 seconds on “Why you should care.” These 35 seconds should be entirely dedicated to describing the buyer’s pain points and how you solve them. At ADLM, buyers spend an average of only 2–3 minutes at each booth; if you can’t capture their attention within the first 60 seconds, they’ll move on to the next booth.
Finally, regarding post-show follow-up, this is the most overlooked yet highest-ROI part of the entire ADLM experience. Statistics show that over 70% of business cards and contact information collected at trade shows are never effectively followed up on after the event.The reason is simple: as soon as exhibitors return to their daily work, they are immediately overwhelmed by a backlog of emails and tasks. The key to solving this problem is to establish a 48-hour post-show action plan before the event: by the evening of the final day, the team should have already prioritized all potential partners and leads (A-level: must be followed up within 48 hours; B-level: follow up within one week;C: Enter into the CRM system within one month), and everyone should be clear on the list they are responsible for following up on. On the first day back in the office, follow-up emails for A-level leads should already have been sent—at this point, the other party’s impression of you is still fresh, and the response rate is 3–5 times higher than if sent a week later. If you can achieve a follow-up coverage rate of over 90% within the first 48 hours after the show, your ROI at ADLM will already exceed that of most exhibitors.
In addition to pre-show preparation, on-site execution during the event also requires a systematic strategy. A time-tested method at large-scale exhibitions like ADLM is the “Three-Tier Information Gathering Approach”: The first tier is the “Executive Level”—where CEO or VP-level personnel attend closed-door forums, industry breakfasts, and CEO roundtables to gain strategic insights into industry trends and identify potential strategic partners; the second tier is the “Technical Level”——involves R&D directors or senior scientists actively participating in academic sub-forums and Scientific Poster Sessions to track cutting-edge technological advancements and assess their potential impact on the company’s pipeline; the third tier is the “Business Tier”—where BD and procurement personnel conduct a comprehensive sweep of the Clinical Lab Expo exhibition hall to collect supplier information, obtain quotes, and schedule follow-up technical evaluation meetings.Information from these three tiers is consolidated during nightly team debriefings to generate actionable insights for the day and optimization strategies for the following day. The advantage of this tiered strategy is that personnel in different roles do not get lost in the vast amount of information at the exhibition; everyone knows their core mission, while the team as a whole achieves comprehensive coverage of the event’s information.
6.0 Conclusion: The Unmissable bio convention in Anaheim — The Next Five Years of Biopharmaceuticals as Seen Through ADLM 2026

6.1 Summary of Key Insights: The Boundaries Between Diagnostics and Therapeutics Are Blurring (The Convergence of Diagnostics and Therapeutics)
Let’s return to the Anaheim Convention Center in late July 2026.As you stand on the second-floor walkway of this building, looking down at the densely packed booths and crowds in the main hall below—to your left is Illumina’s new NovaSeq X, to your right is Roche’s BenchMark Ultra IHC staining platform, and in the corner, a business development team from a company called Strand Therapeutics is discussing a “validation protocol for tumor-specific expression of programmable mRNA” with a CDx company.In that moment, you realize—the traditional dividing line between “pharmaceuticals” and “diagnostics” no longer exists.
In the future of biopharmaceuticals, there will be only one unified concept: Theranostics. Throughout a drug’s entire lifecycle, from R&D to market launch, diagnostic tools are not merely “supporting elements” but “infrastructure.” Just as steel and concrete form the foundation of a building while interior design adds aesthetic value—diagnostic technology is the bedrock of the biopharmaceutical industry.Without mutation detection precise to 0.01% allele frequency, you won’t know when your TKI inhibitor fails in patients. Without ADC pharmacokinetic analysis with a LOD at the fg/mL level, your clinical pharmacology report cannot fully describe the drug exposure-effect relationship (PK/PD). Without a milligram-level high-throughput automated IHC platform, your targeted drug won’t be able to identify its patient population.
Strand Therapeutics’ programmable mRNA logic circuit is the best illustration of this trend—a nucleic acid drug that inherently incorporates “diagnostic logic” (detecting tumor-specific microRNA → determining whether to express a toxin protein), blurring the line between “drug” and “diagnostic.”It’s hard to call it “a drug requiring a companion diagnostic,” because it is, in fact, “a drug that diagnoses itself.” This represents the most profound paradigm shift in the biopharmaceutical industry in 2026—drugs no longer passively await diagnostic results to guide their use; instead, they actively “diagnose” and make “treatment decisions” on their own.
Looking back at ADLM in 2026 five years from now, we may mark it as the “first year of the diagnosis-treatment convergence”—not because a single earth-shattering event occurred that year, but because the collective consensus of the entire industry underwent an irreversible shift. Diagnostics are no longer an “external procurement service” for pharmaceutical companies’ R&D departments, but rather a “core component of their competitive advantage.”This shift will redefine pharmaceutical companies’ organizational structures, talent pools, and budget allocations—within the next five years, the proportion of biomarker and diagnostic scientists in the clinical development departments of leading pharmaceutical companies will rise from the current 15–20% to 30–40%.
Take this “Three Circles” model with you to Anaheim, and you won’t get lost in the hustle and bustle of 20,000 people.You’ll know exactly which companies are in your core circle, where they’re located, and who you’re meeting with at what time. You’ll know which technologies in your expansion circle might reshape your pipeline strategy for next year. And you’ll set aside 20% of your time for exploration—because you understand that the best ADLM experience isn’t about “executing your plan,” but about “discovering opportunities beyond your plan while executing it.”
Exploration Circle—your “worth checking out” exhibitors. These are the exhibitors whose relevance you’re unsure of, but whose technologies are intriguing—such as companies doing AI-powered pathological image analysis, startups developing microfluidic organ-on-a-chip technologies, or teams showcasing novel CRISPR diagnostic platforms (for non-therapeutic applications). Allocate 20% of your total exhibition time to the Exploration Circle—unexpected discoveries often come from this group.
Expansion Circle — your “should-see” exhibitors. These do not directly serve your current pipeline but are significant for your next pipeline or for technologies your competitors are using. For example, if you work in ADCs, the Expansion Circle should include Akoya (spatial biology), Quanterix (ultra-sensitive immunoassays), and academic biotech booths showcasing novel mass spectrometry-based immunoassay solutions.
Core Circle — Your “must-see” exhibitors. These are the companies directly relevant to your pipeline.If you are developing nucleic acid therapeutics, the Core Circle includes Oxford Nanopore, Illumina, Thermo Fisher (NGS/QC), Bio-Rad (dPCR), and potential suppliers of targeted modified nucleotides and tool enzymes. Keep this circle to 15 exhibitors or fewer, and schedule appointments before the show.
To help readers navigate a venue with 20,000 attendees, we propose a simple “three-tier” exhibitor screening model:
These five structural shifts are not theoretical speculations but trends already validated by 2025 market data. First, companion diagnostics have evolved from being a “supplement to drugs” to a “prerequisite for drug commercialization.” The clinical trial designs for multiple blockbuster drugs now mandate CDx as a mandatory inclusion criterion rather than an optional one.Second, tightening LDT regulations are reshaping the laboratory ecosystem. Small independent laboratories face soaring compliance costs, which will drive market consolidation toward a few large platform-based CDx suppliers. Third, liquid biopsy technology has reached the critical point for large-scale clinical application, and 2026 will be a pivotal year for the approval of multiple ctDNA testing products.Fourth, the rise of programmable nucleic acid therapeutics is creating an entirely new “nucleic acid therapeutics + CDx” market space; research data from Strand and Replicate represent only the tip of the iceberg. Fifth, the geopolitical trends in global supply chains are redefining the compliance boundaries for raw material procurement; the impact of the Biosecure Act has already substantially altered the supplier screening criteria for U.S. pharmaceutical companies.
Returning to the question posed at the beginning of this article: Is ADLM 2026 worth your time and budget? If your company is involved in any of the following areas—nucleic acid therapeutics, macromolecular drugs, small-molecule targeted therapies, or related diagnostic technologies—the answer is increasingly leaning toward “yes.”Not because ADLM is such a great marketing platform—it isn’t, in and of itself. Rather, given the regulatory environment and market landscape of 2026, ADLM represents a unique signal: as the boundaries between diagnostics and therapeutics blur, whoever can first establish technical and commercial advantages at this frontier will gain a head start over the next five years. Anaheim is not the end; it is the beginning.
From a broader perspective, ADLM 2026 reflects a fundamental redefinition of the entire in vitro diagnostics industry. A decade ago, ADLM (then known as AACC) was primarily defined as “the annual gathering of clinical laboratory scientists.” Today, its identity is evolving into “the proving ground for next-generation therapies”—an industry hub where diagnostic technologies, drug development, and commercial strategies converge on a single platform.This identity shift is no accident; it is driven by three irreversible structural forces: precision medicine’s deep reliance on diagnostic technologies, regulatory frameworks mandating joint approval for diagnostics and treatments, and the global supply chain’s unprecedented emphasis on the safety and traceability of diagnostic raw materials.The combined effect of these three forces means that ADLM is no longer just a “nice-to-attend” event, but is becoming a “must-attend” one—at least for any company involved in precision medicine.
Ultimately, ADLM 2026 is less a trade show and more a mirror—one that reflects the profound structural shifts currently underway across the precision medicine industry: diagnostics and therapeutics are no longer sequential steps but two sides of the same coin; biomarkers are no longer merely symbols of statistical significance in academic papers but core commercial assets for pharmaceutical companies; and the supply chain is no longer a back-office support function but a decisive factor in product competitiveness on the front lines.For China’s biotechnology companies, understanding and embracing these changes is not merely about securing more collaboration opportunities at ADLM 2026—it is about securing an irreplaceable position in the global competition for precision medicine. See you in Anaheim.
More importantly, the value of ADLM 2026 lies not only in what it offers but also in the industry signals it reflects.If you examine this year’s conference agenda and exhibitor list closely, you will notice a clear trend: topics previously scattered across different industry conferences—nucleic acid drug delivery technologies, the bystander effect in ADCs, and monitoring of resistance mutations in small-molecule kinase inhibitors—are being woven into a unified narrative by advances in diagnostic technologies.The core premise of this narrative is this: when we can track the molecular-level changes drugs induce in the human body with higher resolution, greater speed, and lower cost, the entire paradigm of drug development will be redefined.Clinical trial enrollment criteria will no longer be based solely on histological classification but on real-time dynamic monitoring of biomarkers; drug dose optimization will no longer rely on population-average data but on real-time, individualized feedback adjustments; and the emergence of drug resistance will no longer be an unexpected event but can be predicted in advance through regular liquid biopsies. These changes are already underway, and ADLM 2026 offers the best window to observe and participate in them.
6.2 Next Steps for Readers: How to Use This Outline to Create Your Personalized ADLM 2026 On-Site Strategy
This is a long article—if you’ve read it from start to finish, you already hold a greater “information asymmetry advantage” than 90% of ADLM attendees. But information alone has no value; action does. Below is the “ADLM 2026 Action Checklist” distilled from this article:
Two weeks before the event—finalize your “targeted exhibitor list,” prepare three sets of English talking points, schedule face-to-face meetings at the booths of 10–15 target exhibitors, and connect with key contacts on LinkedIn to warm up the relationship.
Day 1—”Exhibit Hall Tour + Observation.” Avoid in-depth conversations; focus solely on browsing and noting down leads. Attend 1–2 academic sessions on the second floor. Attend 1–2 exhibitor receptions in the evening.
Day 2 — “Targeted Visits + In-Depth Discussions.” Visit 10–15 target exhibitors in order of priority. Engage in conversation with 2–3 technical staff members at each exhibitor’s booth (don’t limit yourself to just one person). Attend an alumni or hometown gathering in the evening.
Day 3 — “In-Depth Meetings + Follow-Up.” Schedule in-depth off-site meetings with 2–3 companies showing the greatest potential for collaboration. Catch up on any important booths you missed on Days 1 and 2. Attend the final academic session.
One Week After the Event — “Summary + Follow-Up.” Organize all collected business cards and technical materials. Send personalized follow-up emails to every company with “potential for collaboration” (mentioning specific details from your conversations at the event). Update your supplier evaluation matrix (the three-dimensional table covering stability, cost, and TAT).
July 26, 2026, Anaheim. This Southern California city, famous for Disneyland, will transform into a global “judging arena” for the biopharmaceutical industry for five days—everyone is being “judged” (Is your technology robust enough? Is your pricing competitive enough?Is your compliance system sufficiently globalized?), and everyone is “judging” others (Can this supplier become the “infrastructure” of my pipeline?). If you haven’t booked your hotel and flights yet—do it now. Hotel rooms in Anaheim for late July are typically fully booked by the end of May each year.
Table 6.1: ADLM 2026 On-Site Roadmap—Timeline and Action List
| Milestone | Action Item | Key Deliverables | Notes |
| 2 Weeks Before the Event | Targeted exhibitor screening + preparation of talking points + scheduling of meetings | List of 15 target exhibitors + meeting confirmation emails | Scheduling emails must specify technical requirements; do not send templates |
| 1 Week Before the Event | LinkedIn engagement + conference registration + hotel and flight confirmations | Connect with 30 target contacts + conference schedule | Register for the Scientific Meeting (not just the Expo) |
| Day 1 (July 26) | Expo Tour + Academic Sessions + Evening Reception | Exhibitor Checklist + Session Notes | Avoid deep conversations; bring plenty of business cards; wear business casual attire |
| Day 2 (July 27) | Targeted Visits + Evening Alumni Gathering | Records of visits to 10–15 exhibitors | Speak with 2–3 people at each booth; get the Applied Scientist’s phone number |
| Day 3 (7/28) | In-depth meetings + follow-up + final academic session | Notes from 2–3 in-depth meetings | Bring pipeline data (non-confidential); meetings in the hotel café |
| 1 week after the meeting | Compile materials + send personalized follow-up emails + update evaluation matrix | Follow-up emails sent + Supplier Matrix v2 | Do not send mass emails; mention specific conversations from the event |
7.0 bio convention FAQ: Frequently Asked Questions About ADLM 2026

Below are the five most frequently asked questions by attendees and industry professionals leading up to the event. Based on our in-depth research into this year’s ADLM, we provide direct and practical answers.
Q1: What are the specific dates and location for ADLM 2026? How do I register?
ADLM 2026 (Association for Diagnostics & Laboratory Medicine Annual Scientific Meeting & Clinical Lab Expo) will be held from July 26 to 30, 2026, at the Anaheim Convention Center in Anaheim, California, USA.The Scientific Meeting will take place from July 26 to 29, and the Clinical Lab Expo will run from July 28 to 30.
There are three types of registration:
① Full Conference Pass: Includes access to all academic sessions and the Expo. Price: approximately $700–950 (early bird and member rates vary).
② Expo Only Pass: Grants access to the exhibition hall only; price ranges from approximately $200 to $350.
③ One-Day Pass: Limited to academic sessions on a specific day; price approximately $350–500.
Registration is completed on the ADLM official website (www.myadlm.org). If you are attending on behalf of a pharmaceutical company, we strongly recommend registering for the Full Conference Pass—the value of the academic sessions is at least three times that of the Expo. If your focus is on procurement and supply chain networking, the Expo Only Pass combined with the evening reception may offer the best value.
Q2: I’m not in diagnostics; I’m in pharmaceuticals—is ADLM really useful for me?
If you hold one of the following roles at a biotech or pharmaceutical company—Director/Manager of Clinical Development, Translational Medicine Scientist, Biomarker Lead, VP of Early-Stage R&D, or CMC Quality Lead—ADLM is valuable to you. Moreover, at this juncture in 2026, it may be the most efficient “three-day information accelerator” available to you on a global scale. Here’s why:
① Your drug requires a “patient screening strategy” (biomarker strategy) during the IND phase—the ADLM Expo is the world’s largest centralized showcase for companion diagnostics.
② Your drug requires “efficacy biomarkers” during the Phase I–II clinical stages to demonstrate target engagement—ADLM’s Scientific Meeting features reports on the most cutting-edge analytical technologies.
③ Your drug requires quality control tools during the CMC phase (especially for nucleic acid therapeutics and ADCs)—the ADLM Expo covers the full range of QC equipment and consumables, from sequencing to mass spectrometry to capillary electrophoresis.
④ Your drug requires a “bridge” for a companion diagnostic strategy supporting simultaneous US and China submissions—at ADLM, you can engage directly with regulatory advisors with FDA review backgrounds, representatives from multinational IVD giants, and Chinese CRO/CDMO representatives to align the perspectives of all three parties in a single meeting.
Q3: When will Strand Therapeutics and Replicate Bioscience’s programmable mRNA enter clinical trials?
As of Q2 2026 (June), both Strand Therapeutics and Replicate Bioscience are in the IND-enabling (clinical trial preparation) phase and have not yet formally submitted IND applications. Based on the progress publicly disclosed by both companies in Q1–Q2 2026:
① Strand Therapeutics has completed GMP-grade process validation and the first GLP toxicology study for STR-001 (its first solid tumor mRNA candidate). It expects to submit an IND application to the FDA in Q3–Q4 2026. If the review proceeds smoothly (with no clinical hold), the first patient enrollment (FPI) could occur in H1 2027.
② Replicate Bioscience’s self-replicating RNA (srRNA) oncology pipeline has completed a dose-escalation study in non-human primates (NHPs), with data published in *Molecular Therapy* in April 2026. The IND submission is expected between Q4 2026 and Q1 2027.
③ The core technology of both companies—“logic circuit-based tumor-specific expression”—has demonstrated impressive data in preclinical models; however, the human tumor microenvironment is far more complex than PDX mouse models. Preliminary signals regarding safety and efficacy in humans may not be observed until 2027–2028.
Q4: Are Chinese nucleic acid raw material companies competitive in the ADLM market? How should they enter the market?
They are competitive, but the competition is not about “who is the cheapest.” The quality standards of Chinese companies in categories such as modified nucleotides, tool enzymes, and plasmid DNA have improved significantly over the past three years—several companies have already obtained FDA DMF filings and passed supplier audits by multinational pharmaceutical companies. The true competitive advantages lie in three areas:
① Category Focus—It’s not about “we can do everything,” but rather “we rank among the top five globally in the single category of modified nucleotides.”
② Response Speed—We can complete the process from inquiry to sample delivery in 2–3 weeks (compared to 6–8 weeks for European and American suppliers).
③ Supply chain transparency—We are open to third-party quality audits of our facilities and provide a complete quality data chain, from raw material traceability to the final Certificate of Analysis (COA).
In terms of market entry strategy, avoid directly challenging U.S. suppliers’ existing customer relationships. A smarter approach is to target small and medium-sized biotech companies in the IND-enabling phase who are establishing their first GMP supply chain—unlike large pharmaceutical companies, these firms do not have fixed supplier lists, are more price-sensitive, and are more open to trying new suppliers. ADLM is the ideal venue for identifying these “unlocked buyers.”
Q5: If I’m only attending ADLM for one day, how should I plan my schedule to get the most out of it?
Attending for just one day is a “highly efficient but risky” strategy—you’ll need exceptional discipline and must not waste more than five minutes at any booth or on giveaways. Here’s the recommended “one-day intensive itinerary”:
① 8:00–10:00 AM: Attend the two morning Keynote/Plenary Sessions. Choose topics most relevant to your field (nucleic acid analysis, ADC biomarkers, liquid biopsy, LDT regulation—depending on your role), prioritizing academic knowledge acquisition.
② 10:00 AM–1:00 PM: Quick tour of the exhibition hall. Do not spend more than 10 minutes at any single booth. Goal: Quickly identify 3–5 exhibitors worth returning to for in-depth discussions.
③ 1:00–2:00 PM: Lunch + Organization. Rank the 5 exhibitors you flagged this morning by priority. Use the ADLM app on your phone to check their booth locations and plan the most efficient walking route.
④ 2:00–5:00 PM: In-depth visits. Visit only the 3–5 exhibitors you selected. At each booth, find their application scientist (not a salesperson) and engage in a deep discussion using the pre-prepared “3D Evaluation Framework” questions.
⑤ 5:00–7:00 PM: Attend at least one evening reception. The ROI from networking here may be higher than during daytime hall interactions—avoid discussing work at the reception (they’ve been hearing about it all day), and instead talk about industry trends, technological advancements, and your thoughts on their latest paper. Relationships built in a relaxed atmosphere yield 3–5 times higher response rates for follow-ups.
If you strictly follow these five steps, the density of “information intake and networking” you can achieve in a single day may surpass that of many “conference-hoppers” who spend three days wandering the exhibition hall. Of course, this assumes—you actually followed them strictly and didn’t get distracted by a booth’s big screen and free coffee during Step 2.
Table 4.3 Comparison of Commercialization Progress for Sample-to-Answer Platforms (2025–2026)
| Platform Name | Year of Release | FDA Status | Core Advantages | Key Limitations |
| BioFire FilmArray 2.0 | 2023 | Approved | Results in 15 minutes, multi-array parallel processing | Supports only pre-defined targets |
| Cepheid Xpert Xpress | 2022 | Approved | Compact design, suitable for POC settings | Slow target expansion |
| Roche cobas pure | 2025 | Under registration | Fully automated sample processing and testing | European market only |
| Qiagen QIAreach | Q2 2026 | Clinically validated | Digital PCR + Smart Software Integration | Not yet CE-IVD certified |
| Hologic Panther Fusion | 2024 | Approved | High-throughput, multipathogen parallel testing | Higher equipment costs |
Table 5.3 Comparison of CDx Regulatory Requirements in Major Global Markets for 2025–2026
| Regulatory Considerations | U.S. FDA | EU IVDR | Japan PMDA | China NMPA |
| CDx Product Classification | Class II/III | Class C/Custom-made | Clinical Testing Instruments | Class III In Vitro Diagnostic Reagents |
| LDT Regulation | Effective Q3 2026 | Not applicable | Not applicable | No clear regulations yet |
| Clinical validation requirements | IDE or de novo 510(k) | Performance evaluation + CE marking | Single-site or multi-site validation | Clinical trials |
| Approval Timeline | 6–12 months | 12–18 months | 12–24 months | 12–18 months |
| Submitted in conjunction with a companion drug | Support for PMA | Supports concurrent review | Supports concurrent review | Supports joint review |
When developing your ADLM attendance strategy, we recommend using a “three-tier screening” approach to identify your target booths and forums. The first tier is “Core Must-Sees“—booths and forums directly related to your business, which you must visit in person. We suggest listing 3–5 of these. The second tier is “High-Value Optionals“—new technologies or partners with indirect relevance to your business, which you should visit if time permits.List 5–10. The third tier is “Intelligence Gathering”—booths of key competitors and industry panel discussions. Assign a team member specifically to visit these locations to gather information. The core logic behind this three-tier screening is to ensure the quality of execution for core objectives while not missing out on unexpected opportunities.
One final recommendation: Complete post-show follow-ups within 48 hours of the event’s conclusion. ADLM attendees have the highest response rates within two weeks of the show, after which rates drop rapidly.For every business card collected at the event, send a first follow-up email within 48 hours—not a templated “Thank you for visiting,” but one that references specific details from your on-site discussion and includes a clear call to action (such as “Schedule an online demo”). This personalized approach yields 3–5 times higher conversion rates than standardized post-show marketing processes.
If you decide to attend the event in Anaheim, the next 12 months are a golden opportunity for preparation. We recommend organizing your ADLM 2026 preparations according to the following timeline: Complete exhibitor registration and booth booking by April 2026—booths along the main aisle of the South Hall typically sell out within six weeks of registration opening.April–May: Begin researching and inviting target clients—use LinkedIn Sales Navigator to identify BD and R&D VPs at pharmaceutical companies that have confirmed their attendance, send personalized one-on-one invitation emails, and schedule 15-minute in-person meetings during the event.May–June: Finalize booth design and prepare demos—ensure technical demonstrations can run independently without an internet connection, as the Anaheim Convention Center’s Wi-Fi is often unreliable during peak exhibition hours.Mid-June: Complete the team’s trade show training—every booth staff member should be able to independently conduct technical presentations and demo demonstrations, while also knowing how to answer common questions regarding compliance certifications, delivery timelines, and pricing structures. One week before the show, send final confirmation emails to all scheduled meeting attendees. The core principle of this timeline is: the greater the lead time, the stronger the on-site execution.
For companies that are not exhibiting but plan to attend ADLM as visitors, the strategy differs but still requires advance planning. Visitor registration typically opens one month before the event, and early-bird registration fees are 40–50% cheaper than on-site registration. More importantly, visitors can use the official ADLM app to browse the exhibitor directory and conference agenda in advance, bookmark booths and forums of interest, and book one-on-one business meeting slots.This feature saw extremely high usage rates when it was first introduced in 2025—visitors who pre-registered completed 2.8 times more valid business contacts during the event than those who did not. For Chinese SMEs with limited budgets, attending as a visitor may be a more cost-effective entry point: spending 3–4 days to fully understand the market, build networks, and gather intelligence, thereby accumulating first-hand data to inform next year’s decision to exhibit.
If your company has not yet decided whether to exhibit at ADLM 2026, here is a simple ROI calculation framework for your reference. Assuming total exhibition costs (booth fees, travel expenses, materials, and personnel costs) are approximately $80,000–$120,000, you will need to secure at least 3–5 high-quality business contacts through the exhibition to cover these costs.A “high-quality business lead” is defined as a lead that progresses to substantive business negotiations within six months of the show. Based on post-show data from ADLM 2025, on average, approximately 8–12 out of every 100 booth visitors will enter substantive business negotiations within six months of the event.If your booth design, demo presentations, and team can increase this ratio to 15% or higher, then during the three-day ADLM exhibition, you only need to host 200–300 visitors to reach the ROI break-even point. Considering that the average daily foot traffic at ADLM is 300–500 visitors, achieving ROI break-even is not difficult for a well-prepared Chinese company—the key lies in the quality of execution.